Described well in this British Medical Journal investigation, the pharmaceutical industry have captured our medical product regulators. None more so than in Australia, where the Therapeutic Goods Administration (TGA) receive 96% of their budget from the industry they are employed to regulate! As a consequence, it is extremely rare for any product presented to them to not be approved. Doctors I know have described the fanfare of new drugs promoted to them, and then the silent disappearance of those drugs into the ether as they are rejected as useless and/or harmful. In the interim, massive amounts of profits are made and who knows the impact on public health as chronic diseases and auto-immune conditions escalate.

In response to this capture, many thousands of doctors and scientists are fighting back. As an example, the NZDSOS team include some named and many anonymous doctors and scientists. Others are working independently and anonymously, eg A Midwestern Doctor writes on The Forgotten Side of Medicine; Australia’s anonymous MD/PhD Dr Ah Kahn Syed writes at Arkmedic’s Blog. I also follow two Canadians, MD/immunologist/nuclear medicine specialist Dr William Makis and PhD/Post-doctorate Dr Jessica Rose, whose CV is one of the most impressive you’ll ever see.
Dr Rose and Dr Syed appear to belong to the ‘Jikkyleaks’ team on Twitter who continually expose data which would normally be monitored and responded to by a functioning regulator. For context, they have a huge issue with Viki Male (@vikilovesfacs), an Imperial College London immunologist who tweets persistently about how “safe and effective” the covid injectables are in pregnancy. Arkmedic has written a two part series on her conflicts of interest/corrupted background (Part 1, Part 2). Her institution are a large recipient of Gates Foundation money; her father owns a patent on the lipid nanoparticle technology; etc etc.
The latest revelations from Jikkyleaks are extremely concerning for women’s health. Copied below from this thread (with some edits to make it more readable in article form).
A new search of the GP prescribing database confirms a MASSIVE safety signal for fertility risk following the COVID vaccine rollout. The one that @vikilovesfacs told you had no impact on fertility. Well check the next tweets and then decide.
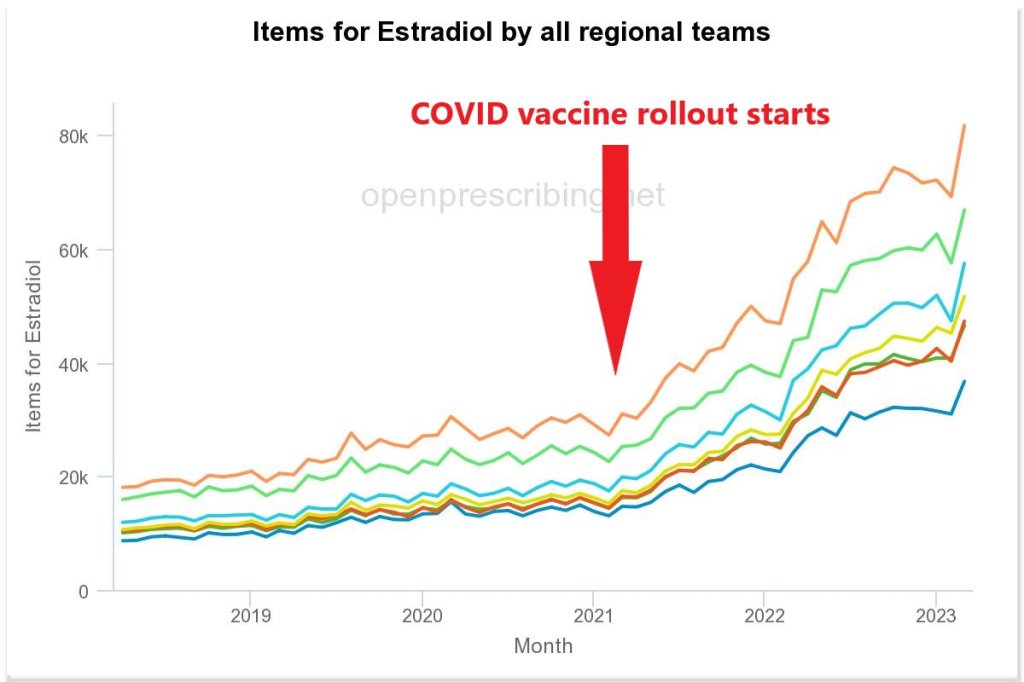
Here it is. The drug which skyrocketed in prescriptions after early 2021 was Estradiol. HRT. Why would this drug suddenly be prescribed in rapidly increasing quantities, having been at a steady level for YEARS following its fall from grace? https://openprescribing.net/chemical/0604011G0/
Of course the answer must be #ClimateChange. One of the primary symptoms of menopause is hot flushes, and these are worse when it’s warm. So that must be it. Global warming (even though it’s getting colder). It cannot possibly be anything else that happened in early 2021.

What it definitely can’t be is anything to do with the global injection of an irritant lipid nanoparticle that was known to accumulate in the ovaries, containing RNA encoding for a foreign protein. No. Absolutely not.
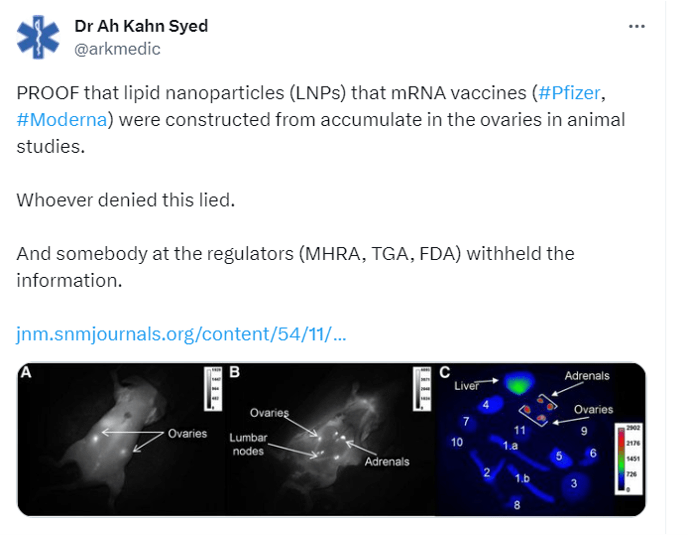
Because if the world was injected with such an irritant or toxic product that went to the ovaries and potentially caused premature ovarian failure as a result, the regulators such as the @MHRAgovuk @TGAgovau and @US_FDA would have told us. Wouldn’t they?

And they would have noticed that an early safety signal for such an event (premature ovarian failure) would have been a sudden increase in the prescribing of HRT. Hormone replacement therapy. Estradiol. And the pharmacovigilance people would have halted the rollout, no?
Of course we have been here before. In the 1970s the pharma companies thought they had “cured” the menopause by dishing out estradiol to as many women as possible. And then the uterine cancer epidemic happened. If this happened today, nobody would be allowed to speak out.
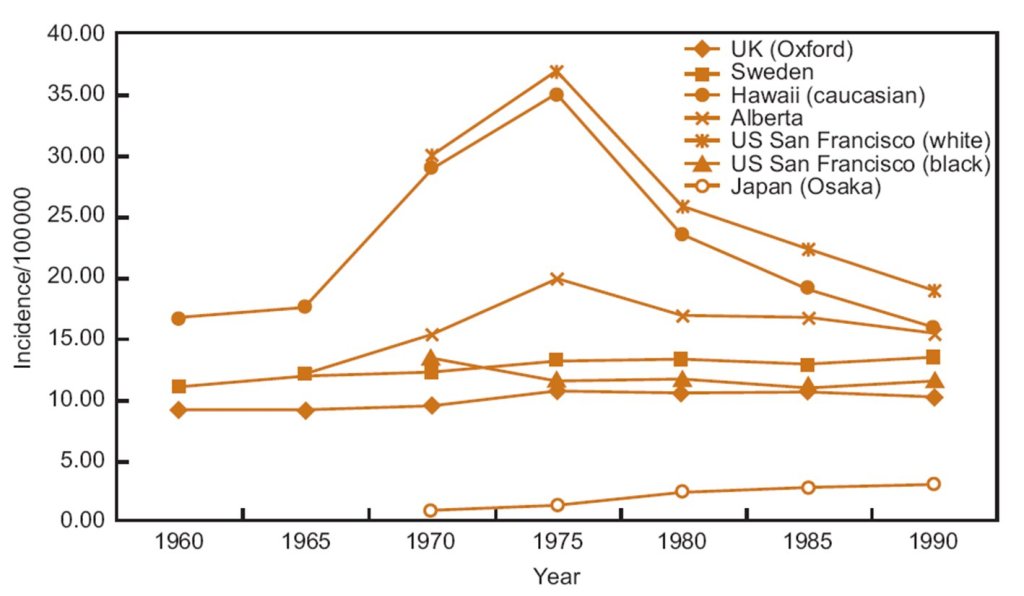
The point is that estradiol is not prescribed routinely. It is not contraceptive estrogen. The days of routinely prescribing HRT for “menopause” have gone since the Women’s Health Initiative study showed a higher rate of heart disease and breast cancer.
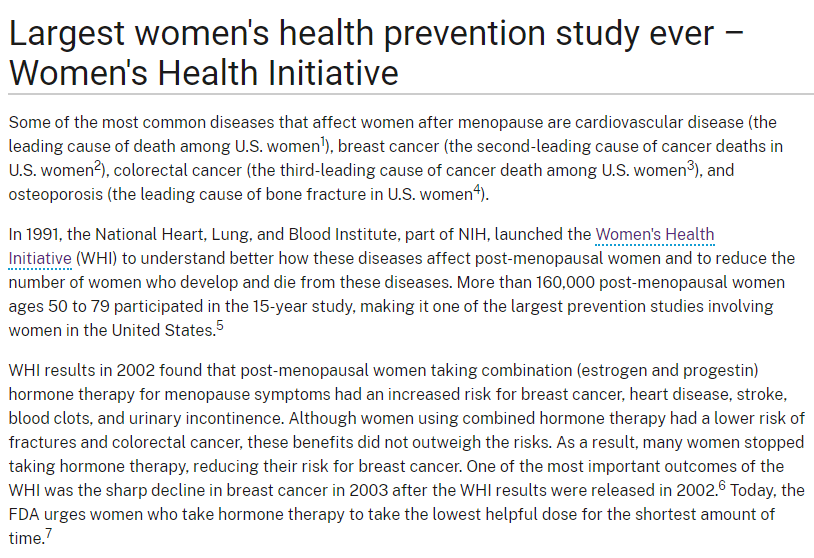
That was 20 years ago and apart from the pharma shills like @drjengunter pushing it excessively, prescriptions for HRT – especially in the UK – are low level and very stable. That’s because the risks usually exceed the benefits over age 50.
So a TRIPLING of the prescription of HRT would be unprecedented. And no, it’s not climate change. It can only represent one thing – that women *under 50* are suddenly being prescribed HRT in record amounts.
And this could only happen if a cohort of otherwise healthy women in their 40s (because the over 50s would be expected to enter menopause) suddenly found themselves in an early menopause. The GPs wouldn’t hesitate to prescribe HRT in that situation. Which means….
This massive and unprecedented spike in HRT prescribing, most notable in the South East region, is due to something that happened to females aged 40-50 from March 2021 onwards that caused premature ovarian failure in unprecedented numbers.
And you can tell that the story needs to be buried because the Pharma-controlled media and their “celebrities” are pushing a new drive for hormone replacement therapy. So that they can blame the massive rise in prescriptions on “increased awareness”.
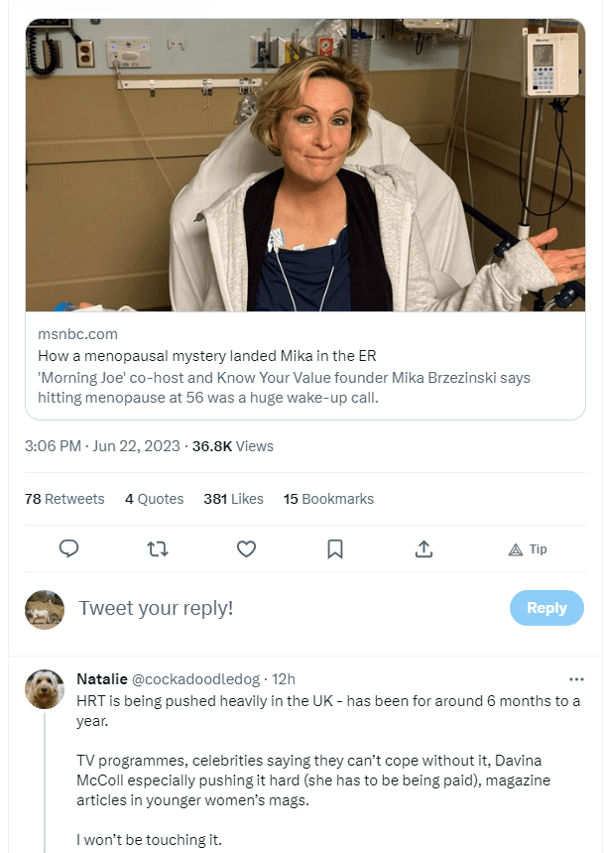
But it’s another distraction and those individual women going to their GP having a sudden menopause a few years early will just be fobbed off that “it’s normal”. Well, it isn’t… and almost certainly the bigger issue is in the next tweet.
Which is, that if a whole cohort of 40’s women are suddenly entering premature menopause… What is happening to women under 40 who wanted to get pregnant? Well, we know the answer don’t we?
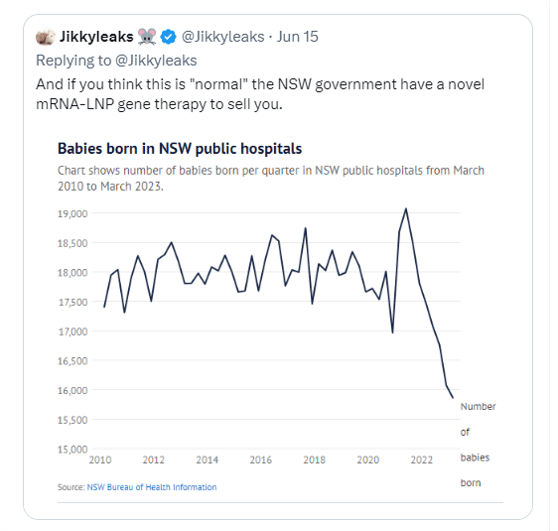
And remember that
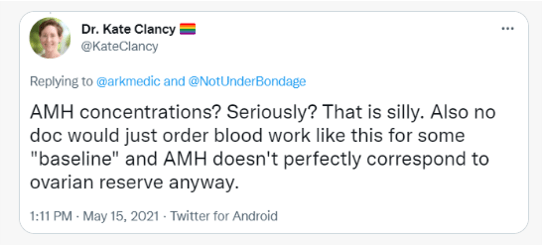
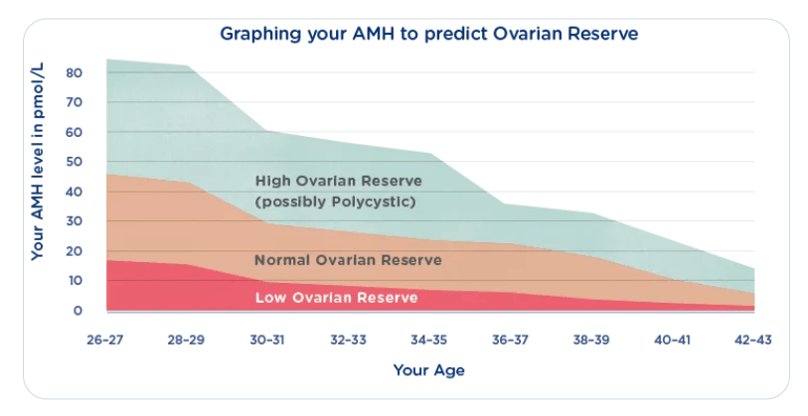
@KateClancy, who pretended to be looking at this very issue, went on a rant when it was suggested two years ago that women could check their AMH levels before engaging on the COVID therapies. Who was she protecting?
The one saving grace here is that the disaster that has afflicted this newly menopausal cohort of women, if treated with any seriousness at all, could help save the fertility of those not yet affected. By warning young women not to take these drugs without more data.
And if you are a young woman who might one day in the future want to get pregnant, speak to your doctor about an AMH test. It could possibly save your fertility.
UPDATE: In typical fashion Viki Male posts a paper almost in unison with this thread to suggest that the AMH values are unaffected by the jabs (when tested early on without boosters). But the paper is a sham. The data is not available to inspection and the estradiol data above proves that there is a major problem, however much the pharma companies try to obfuscate. These papers that Viki quotes are always locked to inspection, because the authors know that we will find inconsistencies in the data that show that they are either biased, misrepresented or in some cases outright fraud.
Groups of doctors and scientists working to fight against this capture of public health (from memory – not an exhaustive list).
Pandata (international)
World Council for Health (international)
Doctors For Covid Ethics (Europe)
HART Group (UK)
Australian Medical Professionals Society (Aus)
Lighthouse Declaration (Aus)
NZDSOS (NZ)
The Health Forum NZ (NZ)
Canadian Covid Care Alliance (Can)
Dr Denis Rancourt (Can)
Frontline Critical Care Alliance (USA)
Americas Frontline Doctors (USA)
Truth for Health Foundation (USA)
