Before leaving Cambodia I did some training with my local colleague on how to correctly weigh babies. She has since trained one of our village volunteers. Last night they sent me some weights from the past few weeks to interpret and advise on. Before I even analyse the results properly, I can see a range of malnutrition issues that are difficult to resolve with our tiny budget and the absence of services. Still it was great to see my butcher scales being put to good use without me and to remain included in their activities from afar.

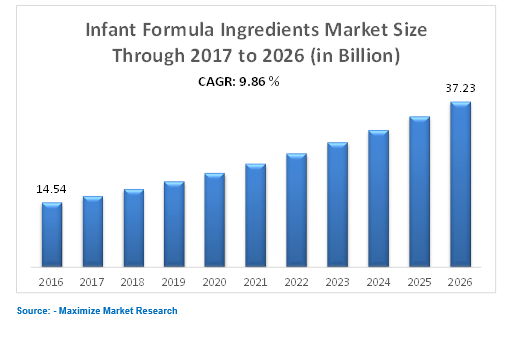
Babies who are breastfed fare better in infancy, but also throughout life, for many reasons connected to the health-giving benefits of breast milk, especially when the baby receives nothing else in their first six months of life. A midwife friend is always talking about the need to “normalise breastfeeding”, because it is up against some serious interference. Many in Australia, for example, consider breastfeeding in public to be improper, with all kinds of cultural constraints placed on young mothers. Bigger than this however, are the various strategies used by corporations to promote breast milk substitutes inside a product market worth billions of dollars and growing steadily. These profits come at a far greater human cost, presenting as infant illness and death in the poorest parts of the world due to multitudes of factors including maternal illiteracy, lack of access to clean water, and substandard or absent health care to teach and support mothers.
In 1981 the World Health Organisation introduced the International Code of Marketing of Breastmilk Substitutes (known as “The Code”), as a policy to protect and promote breastfeeding. The Code consists of a list of recommendations aimed at halting the impact that marketing of breastmilk substitutes is known to have on maternal and child health outcomes, and ultimately on overall public health. When I learned about The Code 20 years ago I, like many others, believed its implementation had resolved the problem. Only my time in Cambodia over the past five years has revealed that in fact The Code is openly violated in a variety of ways, in places with the weakest systems, where population health outcomes are negatively impacted the most.

After learning about these issues years ago during my public health studies, it is only recently that I encountered the reality of them, when I offered a voluntary child health service in a small community in Cambodia. Almost daily I faced situations which led to surprised thoughts such as “I read about this in 1999!”, or “So that’s how a mother who cannot read and write, exposed to milk formula advertising, interprets what she should be doing for her baby”. When I recommended to one young mother of a newborn to “breastfeed your baby until he is six months old, and don’t give him anything else”, she replied “I have no choice because I don’t have money to buy formula”. I applauded her poverty as being a great protection for her baby, causing her to look at me quizzically. The following day during a health education session, a group of mothers announced in unison “we don’t have the money to buy baby milk so we have no choice but to breastfeed”, and again when I greeted their announcement with approval, they seemed taken aback.
There are no lactation services so another young mother described her experience of worrying that she didn’t have enough milk, watching her baby lose weight and having no choice but to persevere under highly stressful circumstances, with no way of seeking advice or support. Her outcome was a success story, no thanks to her poverty preventing her from accessing appropriate support, but simultaneously thanks to her poverty giving her no choice but to “stick it out” with breastfeeding.
The number of mothers in Australia who seek breastfeeding advice and support and the services available here show how important such services are and highlight why, in the absence of services, mothers resort to all sorts of alternative ideas. These alternative ideas may come from ill informed or outdated grandmothers or neighbours, or by paying for services who are being compensated by milk formula companies. Returning this week to Child Health work in Australia, where regulations are in place to protect breastfeeding as the healthiest option and a range of coordinated public health services are available to back this up, the difference in our educated and well-serviced population dazzles me. Feeding breastmilk substitutes in the Australian context comes with far less risk as we have easy access to clean water, a mostly-literate population, health promotion notices on our television screens and high quality health services.
Why would mothers in poor countries where breastfeeding has been the cultural norm be so convinced that breastfeeding is not best for their children? Years of health research tells us a part of the answer to this question, well summarised in this article by Hubert Barennes et al as “Breastfeeding is being endangered by the increased marketing of formula and non-formula milk…. The advertising, though attractive, highly convincing and sometimes subtle, is thoroughly misleading. Funds dedicated to promoting breastfeeding are negligible compared to what is available for the advertising campaigns of companies manufacturing <formula and non-formula milk>“. Ellen Piwoz and Sandra Huffman described the impact of this in their 2015 article in which they state “Suboptimal breastfeeding results in 800 000 child deaths annually. There are multiple causes of suboptimal breastfeeding, including marketing of breast-milk substitutes“.
In 1974 an organisation called War on Want published a report titled “The Baby Killer”. This report is not a long read, but four decades on it remains a worthwhile and relevant read. Part of that relevance is the ongoing issue of infant formula and food product companies expanding their markets into communities who are more susceptible to marketing pressures, less protected due to substandard services and absent or poorly enforced regulations, and more vulnerable to the health and economic impacts associated with using breastmilk substitutes.
Stories from The Baby Killer report included trained and untrained staff wearing crisp white nurse uniforms to represent their milk substitute companies and claims from their companies that the role of said staff was “health education”. Yet investigations showed that this education promoted the idea that breastfeeding needed to be supplemented. A lot of scandal revolved around the practice of providing free samples to uninformed mothers who did not know that by the time the free can of milk powder was empty, the option to breastfeed would be severely jeopardised. Free samples essentially “lock in” mothers to many months of purchasing canned milk which they often cannot afford. This encourages them to seek alternatives and make the powder last by diluting it beyond recommendations, placing their children at risk of a multitude of health risks such as malnutrition and kidney disease. The most common problem associated with bottle feeding in poor communities is the much higher risk of infection, especially diarrhoea, due to low quality water and sanitation.
A current university assignment requires me to formulate a research project. When I submitted this topic as a possibility the lecturer was surprised to learn that these marketing strategies are still practiced. When I contacted an Australian midwife for advice after meeting the bottle feeding mother who had been given a free sample of infant formula at the clinic where she birthed her newborn, I got the same surprised reaction. Yet the more I read, the more I learn that these tactics remain widespread in parts of the world where systems to protect breastfeeding are deficient and health services are profit making businesses.
A 2008 British Medical Journal research article described the impact of a “Bear Brand” coffee creamer sold in Laos by Nestle, the company at the centre of The Baby Killer scandal in 1974. Research found that the logo of this coffee creamer led to many illiterate mothers believing this product was a breastmilk substitute. Sold in many rural roadside shops it contains 3.6% protein and 27.3% fat (compared with recommended content for infant formulas at 7-12% protein and 40-54% fat), as well as listing sugar as an ingredient. Nestle used the same logo on sterilised cow’s milk and infant formula products. The authors encountered children admitted to hospital with malnutrition who had been exclusively fed this product, prompting their research. Their findings showed that large proportions of the Laotian population believed this brand to be a breast milk substitute, demonstrating the strength of a cute logo over any written warnings not to use it for bottle feeding. Some years later the researchers described Nestle’s delayed response to warnings about this product logo, and a number of humanitarian organisations have boycotted Nestle for their marketing strategies which continue to jeopardise infant health.

Nestle are only one such company however, and others employ similar strategies to expand their markets to poorer parts of the world where profits can be made. For this reason, during my health education sessions in Cambodia I included the political aspect of infant feeding. I showed pictures of commercial products and infographics of the massive profits being made courtesy of young parents being duped into believing that breastmilk substitutes are superior to breastfeeding and that commercial food in packets or jars are superior to fresh food.
The bottle fed baby who we supply one can of formula per week to, seems to be continuing her pattern of low level malnutrition. Could it be that Mum is making that one can last a whole week because she has no cash to purchase the extra needed? Meanwhile in Australia this week my first baby was a bottle fed two month old showing hints of excessive weight gain. Life involves bouncing between advising on under nutrition in one location, to advising on over nutrition in another. And now I’ve blogged through hours of procrastination, it’s time to rewrite my latest failed assignment on the topic!

Shocked at the logo story…What kind of organisation would deliberately dupe a new mother into using coffee creamer as baby food? The same organisation which dupes a new mother out of her precious breast milk while getting baby hooked on their product, knowing Mum likely can’t afford it, can’t read the instructions and has no clean water? Surely this is the crime of the century.
LikeLiked by 1 person
Thank you for this excellent post Helen. I think that all health services need to constantly be aware of enticements to supplementary feeding. Sadly with increasing numbers of babies born too small or too large (macrosomic as a consequence of hyperglycaemia) so they have greater difficulties in initiating breastfeeding, the promise of an easier artificial solution won’t go away.
LikeLike