Dr Paul Farmer, co-founder of Partners In Health, talks about “oops” health care leading to “stupid deaths”. I have often referred to the destitution seen in Cambodia, caused by people needing to pay from their pockets for all health care costs – that’s “Out Of Pocket Spending”, or “oops”. Health care in Cambodia, and across the poor world, is both expensive and generally poor quality, leading to high rates of preventable suffering (including healthcare-induced destitution) and death, aka “stupid deaths”. Farmer refers to “oops” elements in the US health system, comparing care available in affluent parts of America with the lack of care in impoverished areas of higher need, in this excellent article on global health inequalities. Farmer’s narrations of this tragedy playing out across our globe, including this priceless quote, speak volumes:
I was tempted to record the cause of death as “weak health system for poor people,” “uninsured,” “fell through gaping hole in safety net,” or “too poor to survive catastrophic illness.”
It is easy from the rich world to believe that these problems occur due to low knowledge or inexperience, but in fact my Cambodian colleagues have vast experience, knowledge and skill. The issue lies, as described so succinctly by Dr Farmer, with the quality of systems in place. Without established systems, processes and regulations, then up to date, evidence based and consistent care cannot be maintained. For example in Australia, I must show that I have undertaken at least 20 hours of formal professional development annually, in order to maintain my professional registration which is reviewed and renewed each year. I am required to undertake and maintain regular extra training before I can perform some specific tasks or procedures; to follow certain guidelines and processes; and to document my work in specific ways. When I make an error in practice I am required to report it via a risk management system that considers human error an expected deviation to be addressed through quality improvement reviews. These regulated requirements are constantly reviewed and improved in order to ensure that the systems, established to ensure quality care is provided, have intended impact. This ongoing process is what makes the care I provide consistent against the care someone else in a similar job would also provide, which gives service users an appropriate level of trust in the care that they receive. Intuition develops with experience and enhances competence but the same knowledge and experience freely gliding along solo with only individual intuition as a guide would (and does) result in very inconsistent care, and inferior outcomes for those receiving health care.
Sadly it seems that baby Mary, now 10 months old, is on an oops-like trajectory towards a stupid death. She received three months, or about half, of a course of anti-TB medication, sourced from the black market and administered with only vague adherence to the public health recommendations for treatment of tuberculosis. Her response to treatment was slow at best and she continues to present with repeated respiratory infections and ongoing, although slowly improving, malnutrition. A month ago she developed another respiratory infection and the sole doctor treating her responded by ceasing TB medication altogether, based on his persisting intuition that she does not have TB.
This is an astounding response to a baby who is malnourished with respiratory symptoms – the main ingredients of tuberculous disease. Particularly in a place with high prevalence of TB and when her older sibling is permanently disabled from tuberculous meningitis, demonstrating the presence of infectious TB within the vicinity of this family. If she does have TB then partial treatment is both useless for cure as well as placing her at risk of the bacteria developing resistance to the standard treatments, which is why partial treatment for TB is contra-indicated in all of the literature and guidelines. It was probably an inevitable result in this case, as just another link in the chain of care to be expected from a fragmented, disorganised system with inadequate regulation and no requirement for collaboration or structured public health approaches which are the benchmarks of health systems in countries like Australia, New Zealand and the United Kingdom.
Mary was turned away by the National TB Program when they were not able to “tick every box” required by the Global Fund who supply the anti-TB drugs, before the drugs can be dispensed. This is no doubt required as a way to prevent corruption, by ensuring that only people with clear TB diagnoses receive the drugs, which can end up on the black market where they can be used inappropriately (case in point: Mary). It is an example of a system that needs to be reviewed and amended when those needing treatment cannot access anti-TB drugs. World Health Organisation state that “Ensuring all TB patients have access to free-of-charge life-saving treatment is fundamental to minimizing disease and deaths due to TB“, yet this clearly does not happen particularly for the world’s poorest, who are also those at highest risk of TB disease.
Clear TB diagnosis is not always possible as tuberculosis disease often camouflages itself. Patients sick with TB or whose immunity is suppressed by their illness often test negative to the diagnostic tests. Childhood TB very often presents in atypical ways, making diagnosis difficult or impossible. 70% of TB disease occurs in the lungs but 30% occurs in other body organs. It can affect any organ – I have seen skin TB, ovarian TB, abdominal TB and renal TB, to name a few. Patients with unusual TB presentations often present as if they have cancer and in places where consideration of TB is not well programmed (which is usually places where TB is more prevalent, due to the lack of proper systems), it is not unusual for people to be told they have terminal cancer, which is often an incorrectly assumed cause of death. Or, as I continue to learn, that they have a mysterious illness without the world’s leading infectious killer being considered a possibility. A very stupid death indeed, but the fault of systems rather than individuals.
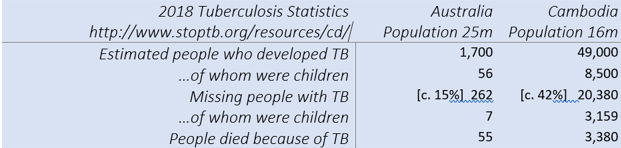
The STOP TB Partnership recently released 2018 statistics per country for TB, at stoptb.org. Below are some comparisons between Australia and Cambodia created from this source. The differences relate specifically to multiple types of poverty, including poverty of living conditions, poverty of health care systems, poverty of population health literacy and poverty of human rights. Less poverty in Australia results in far fewer instances of TB, much less undiagnosed TB when it does occur, and far fewer TB deaths. The estimated TB deaths in Cambodia total almost 10 people per day, most of which occur at the end of an “oops” journey through health services despite claims that TB treatment is free, and all of them “stupid deaths”.

Those stats certainly back up your statement about quality of systems in place. Just another cruelly unfair aspect of poverty.
LikeLike
Here’s an oops moment!
Patient with typical TB signs, symptoms and x-ray lost to follow up for 3 years, working in child care.
https://www.rrh.org.au/journal/article/5552
LikeLike