The First Lockdown
Initially I supported the first ever lockdown in 2020. I believed the fiction of “flattening the curve” in a “pandemic”, although there was always a nagging feeling in the back of my head that something wasn’t quite right. When it became apparent that flattening the imaginary curve was just a segue into keeping society terrorised for as long as possible, I started to search for the reasons that this would be happening.
Information Control
It was impossible to find anything on Google.
In around July of 2020 I somehow found a headline in English quoting microbiologist/virologist Professor Sucharit Bhakdi which seemed sensible, but the actual article was in German, so I was none the wiser. Soon after then I found Professor John Ioannidis, a leading infectious disease epidemiologist at Stanford University, whose research showed that the infection fatality rate of Covid was nothing like the media were claiming. A barrage of articles character assassinating Prof. Ioannidis followed and my nagging suspicions grew, of something being quite wrong.
Weaponised Public Health Was Inevitable
After almost 20 years of working on infectious disease programs, I was acutely aware of the lies that media spread. Many years ago an Australian headline claimed that “HIV in indigenous communities” had “doubled”. The actual figure was that one new case had been diagnosed, making the total cases two. Nevertheless, the headline created social convulsions amongst the populace.
On another occasion a local rag headlined claims from a hospital orderly that he had been exposed to tuberculosis at work and now had TB illness. In fact his positive screening test most likely came from the time he’d spent in the Philippines and he was not sick, he was just prescribed a course of preventive medication.
Examples that I dealt with over the years, highlighting the fact that health professionals do not understand infectious diseases include:
- an infection control nurse claimed she had TB disease and was on treatment. In fact, she had a positive screening test (NOT a disease diagnosis) and was taking preventative treatment.
- a junior doctor who panicked upon learning she’d been caring for a tuberculosis patient prior to their diagnosis. Because she had spent about twenty minutes in the room with this person, she insisted on being screened as a contact despite not meeting the criteria. When her screening test came up positive she was convinced she was sick due to exposure with this patient, when the test could not have been connected to such recent exposure and did not indicate sickness at all.
- a group of paediatricians who claimed a teenage girl with tuberculosis had only a few years to live due to the damage in her lungs. They insisted on being treated as high risk contacts because they’d spent brief amounts of time with her and insisted that their risk was high. No amount of education could settle their frenzy. A few years later that teenage girl’s chest x-ray was completely cleared and she was perfectly healthy. Predictably not one of the paediatricians developed TB. I often wonder if they ever realised how irrational their behaviour was at that time.
During the swine flu non-pandemic of 2009 (when about one third the number of deaths of a normal influenza season occurred worldwide), the media’s non-stop fearmongering caused a mass panic resulting in pressure of public health units to conduct activities that made zero sense but were enacted in order to settle the media frenzy.
So it was always going to be, I guess, that infectious diseases would eventually be weaponised for profit. The level of emotion that they elicit is unmatched. I believe this is one of the main reasons that I changed career paths in 2018, as dealing with the hysterical healthy became increasingly frustrating over time.
Deadly Protocols
The UK government stopped visitation rights of family of elderly care home residents in the name of “covid safety”. At the same time they introduced policies of euthanasia upon those same elderly people. Nice Guideline 163 recommended end-of-life treatments, such as morphine and midazolam. It is believed that many thousands of people whose deaths were recorded as “covid” were in fact euthanased. This issue is covered in the documentary A Good Death? The UK Health Secretary at the time, Matt Hancock, has been nicknamed Midazolam Matt for his criminal involvement which so far, goes unchecked. The case of Derek Dimmock is one example but there are thousands. The scandal remains largely swept under the rug thanks to the complicity of legacy media.
Lockdown as a Weapon

During twenty years of infectious disease surveillance, program management and outbreak control, I never once heard the term “lockdown”. Because it is not a public health intervention. Its introduction as a public health intervention was touted at various simulated pandemic exercises, the most relevant being Event 201 in October 2019, simulating a coronavirus pandemic response just months before Tedros Ghebreyesus announced the Coronavirus pandemic.

Event 201 participants included representatives from the World Bank, the World Economic Forum, Bloomberg/Johns Hopkins University Populations Center, the CDC, various media interests, the Chinese government, a former CIA/NSA director, the world’s larges pharmaceutical company, vaccine maker Johnson & Johnson, finance and biosecurity leaders, and the president of Edelman, the world’s leading corporate PR firm. Conspiracy-minded critics dub this cabal the “Deep State.” The World Economic Forum Director Klaus Schwab has christened their agenda the “Great Reset.” (Reference “The Real Anthony Fauci”).
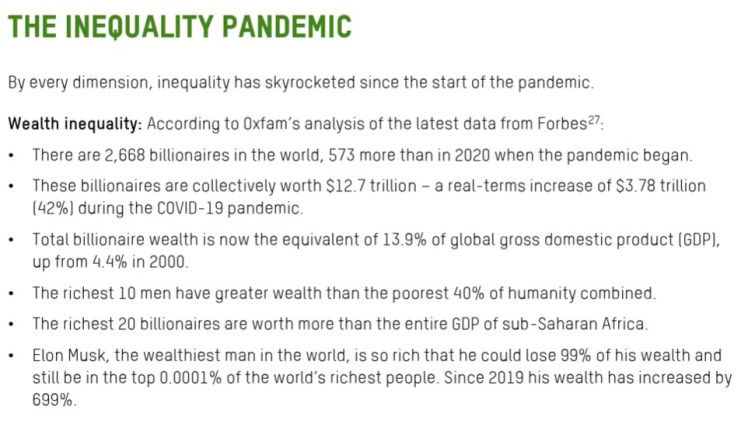
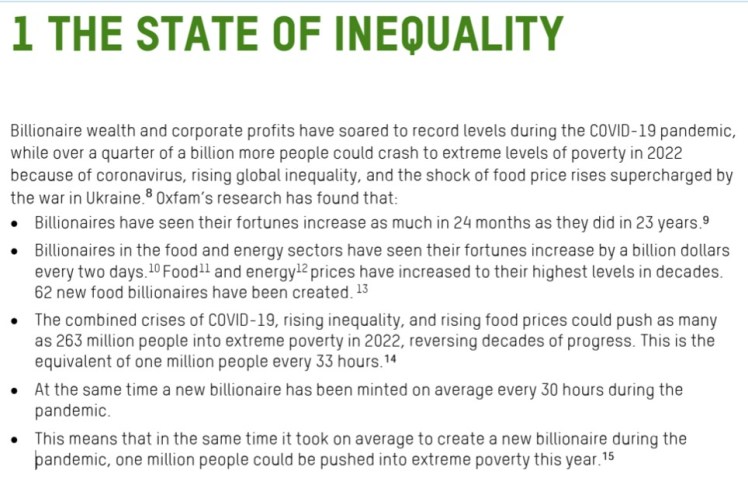
So lockdown is in fact, the product of public-private partnerships. The same partnerships who profit from lockdown via the closure of small businesses, channeling custom to large, centralised corporations, and from the forced consumption of products en masse. The public sector ensure laws and procedures are in place to guarantee maximum uptake of the products. The highly lucrative business model is summarised by Oxfam’s 2022 report Profiting from Pain.
Nipah Virus
This business model is too good not to repeat and so we are very close now, to another series of lockdowns. Over the past four years there have been repeated attempts to convince the public to repeat the fear they felt about covid. Mpox was declared a pandemic by WHO Director-General Tedros in July 2022. It failed to raise enough alarm. Since then, attempts have been made with other infectious diseases, such as Marburg, Bird Flu, Crimean-Congo Haemorrhagic Fever, Measles and a space saved for Disease X, the unknown but guaranteed cause of our next pandemic!
Nipah seems to have taken the lead for now. A faraway land facing a deadly disease which risks the health of us all. In fact, two 25 year old nurses were diagnosed and hospitalised in a region which has regular seasonal cases of Nipah. One of them has already recovered. Contact tracing has resulted in zero linked cases. They live in Kolkata, in West Bengal, inhabited by 100 million people. Where malnutrition and poverty are the actual public health crisis. But malnutrition and poverty don’t bring revenue. Infectious diseases do. As long as the people can be convinced to be adequately afraid.

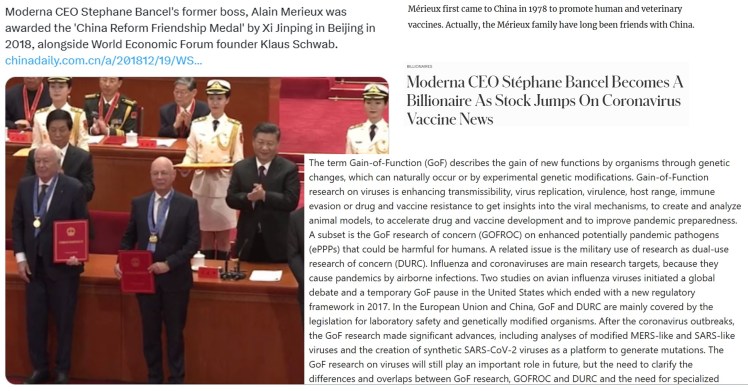
Gain of Function
These are some interesting points to note about Nipah, MPox, and biowarfare research here.
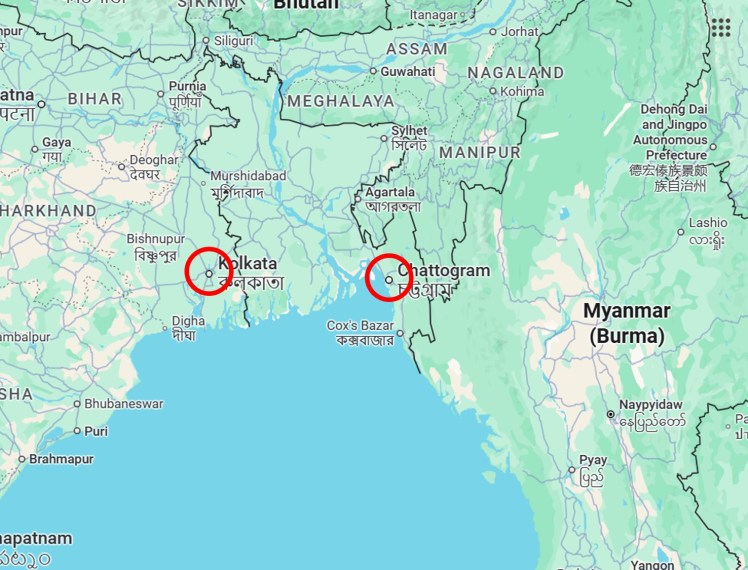
This map shows Chattogram (aka Chittagong) in Bangladesh, and Kolkata in India, both in the region of Bengal. It is a 558km road trip between the two.
More biowarfare research in another third world nation (Democratic Republic of Congo), by the same pharmaceutical company.
This map shows Goma (red marker), in North Kivu Province of the DRC, and Kamituga in South Kivu Province. Kamituga was “ground zero” for the Clade 1B Mpox “outbreak” two years ago. It is a 460km road trip between the two locations.

Some photographs from Kamituga are shared below. World Health Organization Director-General Tedros’ “concern” for these people is MPox. Not poverty. Not drinking water. Not nutrition. Not housing. Not education.
MPox is presented as a “vaccine preventable” disease. The World Health Organization are sponsored by vaccine manufacturers and as such, their role is to market the products. None of the products have been safety tested adequately. Many come with serious safety signals. The effectiveness of the products is under serious scrutiny.
Is it possible that poverty and ill health are being maintained by the actions of the World Health Organization? Could that be why they plan to implement another lockdown on behalf of their sponsors?





