Tuberculosis is an insidious and a complicated disease.
Six years ago I met a young man of about 30 years old who hailed from India. He presented to an Australian hospital with persistent abdominal symptoms. Eventually doctors performed investigations and found multiple lesions on the lining around his abdominal organs. Whilst awaiting results from the specimens taken, he was informed that he had some form of cancer which was probably not treatable, but results would take some weeks. He returned to India to say farewell to his family. While he was away the specimens returned positive to Tuberculosis. The day I met him he had just returned from India and his words to me were “I am only 30 and I believed I was dying! You have no idea how happy I am! They can treat me for TB and I am not dying! It is amazing!”.
A year later I met “Paula”, who I’ve written about extensively. She too, had multiple lesions around her abdominal organ lining. However, she was a poor villager from a remote location in Cambodia. Turning up at a single health service who could investigate her appropriately was not an option. Her experience involved seeking help from multiple services, starting at her village health center and eventually ending up at a tertiary hospital in Phnom Penh. The costs of transportation, paying for various ineffective treatments recommended along the way, accommodation for her family, and hospital fees, had already crippled her family by the time I met them. They had sold their house and were living in the home of a family member. Ultimately her father moved to Malaysia to work for four years, selling doughnuts at a streetside stall, to pay off their health care debts.
In Phnom Penh she was told that she had terminal cancer, and that her life could be prolonged by surgical excision of the lesions. At a cost of thousands, obtained through high-interest loans, abdominal surgery was performed. Part of her intestine was removed and a colostomy was formed on one side of her abdomen. Some sort of surgical error led to a wound forming on the other side of her abdomen, which she described as “oneday it burst open”. By the time I met her, she had two openings on her abdomen, both oozing faecal matter out onto her skin. There were no colostomy bags. She spent her days and nights either applying dressings to contain the faeces, or wiping it away with cloths when they couldn’t afford dressings. She wasn’t able to properly absorb anything that she ate. When I met her in May 2014 she weighed 20.6kg. After intensive therapeutic feeding, some months later the maximum weight she could reach was 25kg.
The reason she turned up at the MSF Tuberculosis service in May 2014, was that alongside her abdominal “cancer”, she also had a productive cough which cultured Tuberculosis bacteria. She had commenced standard anti-TB medications but some weeks later the laboratory tests showed that her TB was drug resistant. She was admitted to our service to commence the much more complicated regime for Multi-Drug-Resistant-TB (MDRTB). The first conversation I had about her, prior to meeting her, was with a doctor who asked me to please admit her and assess her for any muscle mass that might allow us to use intramuscular injections for one of the MDRTB drugs that she needed. She was a skin-covered skeleton and there was no muscle mass, so they treated her with oral drugs only. Soon after commencing MDRTB treatment the abdominal pain she had been experiencing for years, attributed to her “cancer”, disappeared. She would regularly ask us, “Am I going to die?”. She wasn’t going to die from a cancer she never had. Nor from the Multi-Drug-Resistant-TB (MDRTB) that was ultimately cured. But she was going to die from unnecessary surgical complications that left her with a constant ooze of faeces excoriating her abdomen and the irreparable malnutrition that this ooze was responsible for sustaining. It could have all been avoided if TB had been considered when she first presented anywhere.
As insidious and complicated as Tuberculosis is, Tuberculosis in children is a Next Level Felon.
Last year World Health Organisation published this document:
Roadmap towards ending TB in children and adolescents
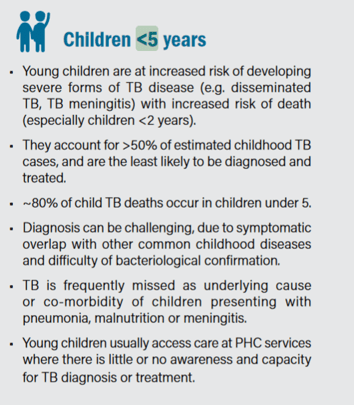
This document describes the difficulties in diagnosing Tuberculosis in children. For example, from Page 1:
“Even though TB is a preventable and curable disease, it continues to impact the lives and development of millions of children and adolescents. Many of the policies and tools needed to break down the continuous cycle of transmission and disease are already in place, but they need to be prioritized, strengthened and fully implemented to move us closer to ending TB.
Latest estimates suggest that 36% of tuberculosis (TB) patients are ‘missing’, meaning that approximately 3.6 million TB patients may not have been diagnosed and properly treated (5). Finding and treating all TB cases – including among children and adolescents – is an urgent operational priority, particularly in high-burden countries”
And from page 8:
What I had not learned until recently when “Mary”, our TB baby in Phnom Penh became unwell, was the bureaucratic layers that prevent children from getting the treatment that they need. In Australia, and on the MSF project where I worked, doctors had the right to make clinical judgements based on a child’s presentation. This is an important aspect to any health service, particularly where childhood Tuberculosis is a differential diagnosis, because the diagnostic tests in children are invariably unreliable. The tests which ask the child’s immune system to respond are unreliable because children’s immune systems are immature and likely to give false negative results. The tests which search for Tuberculosis bacteria in specimens, such as sputum, are unreliable because children can become very unwell with only a tiny number of bacteria present, making it very difficult to find the bacteria on laboratory tests.
However, in Phnom Penh at least, it appears that rules and regulations put in place by well meaning bureaucrats are preventing doctors from treating clinically suspicious paediatric tuberculosis. The systems require various tests to be taken, which on an unwell and tiny baby such as Mary, are inevitably going to return negative. And these negative tests are stopping doctors from using clinical judgement to treat her presumptively for probable TB. The reason for these rules seems to be, preventing corruption – stopping doctors from prescribing TB treatment to people who don’t fit strict criteria. The aim is to stop the precious TB medicines from getting into the hands of someone who may sell them on the Black Market. An unintended outcome seems to be that people sick with TB, especially children, cannot access the drugs that could save their lives. Black Market drugs are not quality controlled, they could be diluted, damaged or expired and are known to contribute to the problem of drug resistance when the bacteria are able to produce enzymes against an ineffective drug.
During my public health studies years ago I learned of the many evils related to the Black Market. I had no idea until very recently that Black Market drugs, as felonious as they are, serve a very real purpose to desperate people with no other choice. Ironically, we are now at a point in time where in order to save Mary’s life, accessing the TB drugs she needs, seems to be only possible via the Black Market!
The real felon in this scenario, which represents many thousands of other TB victims not receiving the treatment that they need, is not so much the Black Market, but the well meaning yet totally flawed bureaucracy.
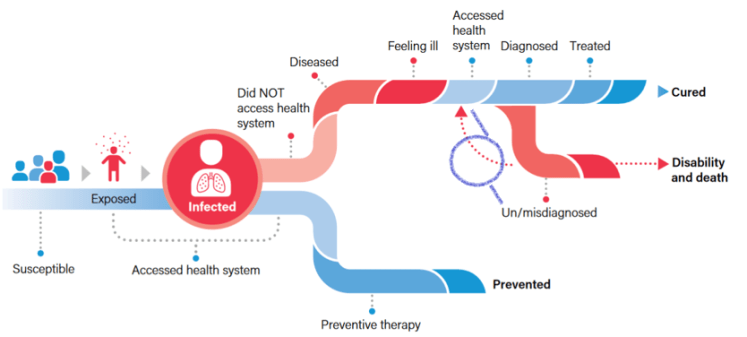
Below is a map of the way that TB does or does not progress in children infected with TB, from page 9 of the Roadmap document. The purple circle and lines between “accessed health system” and “un/misidagnosed” were added by me, showing where in the course of TB disease, Mary is currently at. Returning to health services and being repeatedly turned away without treatment. Perilously close to a disability/death outcome, I hope to be able to report that someone finally offered her treatment, changing her course to treated and cured. * Watch This Space *
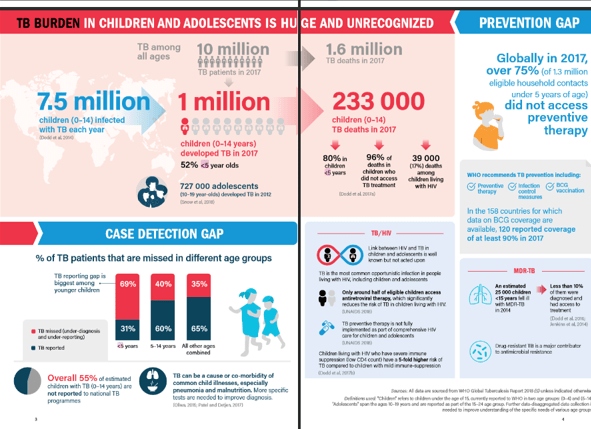
From pages 3 & 4 of WHO’s Roadmap document

It would be nice to think that someone with the right sort of clout & common sense. might take up the cause for this & so many others who need this treatment. Keep up the fight Helen
LikeLike