
One of the first and funniest encounters I had with use of face masks for potentially infectious patients was in 1999 when the hospital ward I worked on accommodated two elderly sisters from a very remote community in northern Australia, who were thought to possibly have Tuberculosis (as it turned out they did not). Because TB is an airborne disease which can cause severe illness and death, they were isolated in a room with it’s own separate negative pressure air conditioning system for a number of weeks while we waited for the results of their TB tests.
An anteroom leading to this isolation room was stocked with Personal Protective Equipment (PPE) including high filtration (N95) masks which staff and visitors donned (put on) as we entered the room and doffed (removed) on exiting the room, disposing of them into a medical waste bin and following strict handwashing procedures before, during and after our interventions. The patients were allowed to go outside and we taught them how to wear their own surgical face masks, which they donned on exit and doffed on entry back into their room.
Despite regular explanations, these delightful sisters never fully understood what we were requesting them to do (wear a blue surgical mask when they left their room) and we frequently saw them walking around in orange high filtration masks, which are required for the uninfected going into an infected space rather than for use by the infected. Oneday a particularly funny sight walked past, where one of them had her mask placed vertically down over her nose and mouth, with no seal at all and the sides of her mouth fully exposed. They regularly wore their masks upside down and inside out, and rarely with any real fit.
Another day I walked into the anteroom to don my N95 mask, which I pulled from its box, and wondered why it was only loosely folded? I realised that our compliant sisters were not only wearing the staff-intended masks, but when returning to their room, they were helping us out by folding them up and putting them back in the box for us to re-use!
This story is an exaggeration of the issues that arise when face masks for preventing infectious diseases are required to be worn. People do all kinds of things, from slinging the mask around their neck and walking it around, exposing it to all manner of microbes before putting it back on their face, to touching it repeatedly without any handwashing, wearing it under their nose or so loosely fitted that it can’t filter any microbes.
A number of studies suggest that cross-contamination when masks are worn in general settings without appropriate training can be more problematic than any protective benefit from wearing masks. This becomes an even bigger problem when people don’t want to wear a mask but feel obliged to do so, as seen with many TB patients who don’t want to comply with the various isolation rules imposed on them during their often lengthy period of infectivity. Even Dr Anthony Fauci, Director of the National Institute of Allergy and Infectious Diseases and one of today’s biggest proponents of face mask use for the general public, did this at a highly publicised baseball game the other night:

Tom Jefferson is a senior associate tutor and honorary research fellow, Centre for Evidence-Based Medicine, University of Oxford. Carl Heneghan is Professor of Evidence-Based Medicine, University of Oxford, Director of the Centre for Evidence-Based Medicine and Editor in Chief of BMJ EBM. They gave an excellent interview on Lockdown TV the other day although when I asked Mum to watch it she informed me that “the bearded gentlemen were quite hard to follow”, (Oxford epidemiologists: suppression strategy is not viable), so it might not be for everyone! They also collaborated on this short piece at the Centre for Evidence-Based Medicine, explaining why so much controversy exists around masks (Masking lack of evidence with politics).
In their rapid review document Should individuals in the community without respiratory symptoms wear facemasks to reduce the spread of COVID-19? the Norwegian Institute of Public Health also describe the confusion.
Health authorities have given conflicting recommendations regarding the use of facemasks by asymptomatic individuals in the community to reduce the spread of COVID-19. For example, the World Health Organization (WHO) states that “at present, there is no direct evidence (from studies on COVID-19 and in healthy people in the community) on the effectiveness of universal masking of healthy people in the community to prevent infection with respiratory viruses, including COVID-19”. Yet, “WHO has updated its guidance to advise that to prevent COVID-19 transmission effectively in areas of community transmission, governments should encourage the general public to wear masks in specific situations and settings as part of a comprehensive approach to suppress SARS-CoV-2 transmission”. This includes settings where individuals are unable to keep a physical distance of at least 1 meter. WHO is also strongly encouraging countries to conduct research on this critical topic.
They go on to describe benefits over risks, specific to the Norwegian setting as at June 2020:
Given the low prevalence of COVID-19 currently, even if facemasks are assumed to be effective, the difference in infection rates between using facemasks and not using facemasks would be small. Assuming that 20% of people infectious with SARS-CoV-2 do not have symptoms, and assuming a risk reduction of 40% for wearing facemask, 200 000 people would need to wear facemasks to prevent one new infection per week in the current epidemiological situation.
The undesirable effects of facemasks include the risks of incorrect use, a false sense of security (leading to relaxation of other interventions), and contamination of masks. In addition, some people experience problems breathing, discomfort, and problems with communication. The proportion of people who experience these undesirable effects is uncertain. However, with a low prevalence of COVID-19, the number of people who experience undesirable effects is likely to be much larger than the number of infections prevented.
How Do Masks Work?
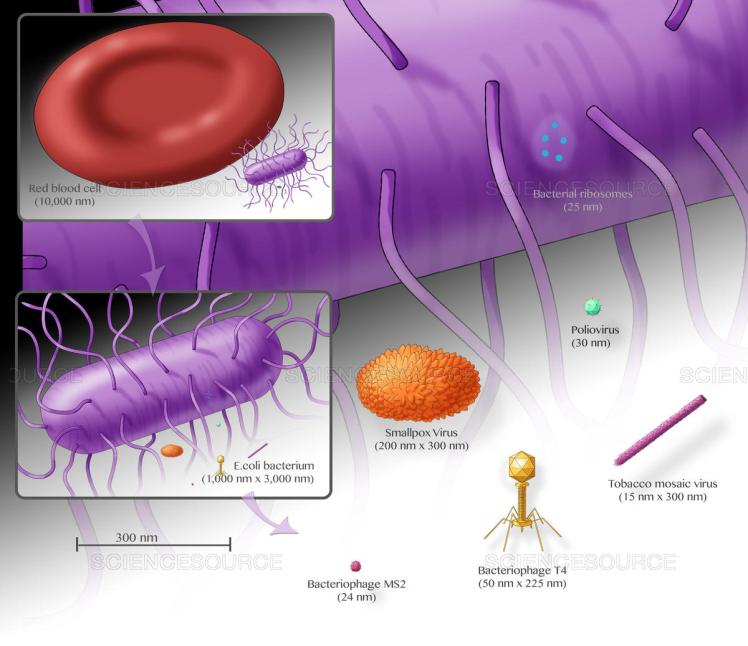
This picture from ScienceSource.com shows some scaled examples of different microscopic sizes. Coronavirus is between 50nm to 200nm, so around half the size of the smallpox virion pictured. Respiratory disease transmission is described as having three different methods, being droplet, airborne and contact.
Droplet transmission occurs when we cough microbes out in large, moist, heavy droplets that fall to the ground quite quickly due to their weight. In this scenario, we need to be quite close to someone infectious to inhale their infectious droplets. Latest advice on Covid-19 is that it transmits via droplet and contact routes with some evidence of airborne transmission in certain circumstances.
Surgical masks are so-called because they were designed to prevent accidental bacterial contamination of wounds by surgeons, as well as to protect the wearer from splashes or sprays of blood or bodily fluid, during surgical procedures. They provide a barrier when worn by an infected person, by blocking large coughed out particles from entering the airspace around them. They are thought to have some protective effect against droplet transmission of respiratory infections, although US Centers for Disease Control state that the evidence is weak for influenza transmission.
Airborne transmission occurs when moist infectious droplets coughed out evaporate or “aerosolise” into lighter “droplet nuclei” and remain suspended in the air for longer periods of time. Far fewer organisms can survive as airborne pathogens, as they need to resist the drying-out that occurs in aerosolisation.
If an organism is transmitted via the airborne route then the tiny droplet nuclei floating in the air space of an infected person will easily pass through the larger filter spaces of a surgical mask. In this instance a high filtration mask is needed for protection of anyone coming into the air space of an infected person. To be effective in any infectious disease setting all masks need to be fitted and worn properly, with a good seal. Mask infection control etiquette includes awareness around touching the mask, which should always be considered potentially contaminated – there’s a reason they’re dubbed “face nappies”; appropriate hand washing; changing them within recommended time frames (before the build-up of breath moisture impairs filtration effect); and proper disposal. When working with airborne pathogens such as Tuberculosis, best practice involves a proper fit test to ensure the correct size mask and to train staff in how to wear them properly.

Contact transmission can occur directly (eg an infected person coughs into their hand, then shakes hands with an uninfected person) or indirectly (eg an infected person coughs on or touches a door handle or a tap, which an uninfected person then touches before then touching their face, presenting the pathogens to ports of entry such as nose, mouth and eyes). Contaminated masks play a part in contact transmission, which is why proper mask etiquette is required.
This segment from the Norwegian Institute of Public Health is a good conclusion to the subject:
Because incorrect use of medical facemasks limits their effectiveness, countrywide training programmes adapted to a variety of audiences would be needed to ensure the effectiveness of medical facemasks for reducing the spread of COVID-19. It is
not known whether the use of medical facemasks would be widely accepted by the healthy population in Norway, or the extent to which correct use could be achieved.
Non-medical facemasks include a variety of products. There is no reliable evidence of the effectiveness of non-medical facemasks in community settings. There is likely to be substantial variation in effectiveness between products. However, there is only limited evidence from laboratory studies of potential differences in effectiveness when different products are used in the community.





