There are so many documents written before 2020 based on public health evidence and advising pandemic response. I have previously shared the WHO Non Pharmaceutical Public Health Measures document. This week I came across this one:
Johns Hopkins University: Preparedness for a High-Impact Respiratory Pathogen Pandemic
Some quotes from this document provide useful insights. The most hard hitting for me is In some cases, implementation of some NPIs, such as travel restrictions and quarantine, might be pursued for social or political purposes by political leaders, rather than pursued because of public health evidence... WHO should rapidly and clearly articulate its opposition to inappropriate NPIs, especially when they threaten public health response activities.
In January when Chinese authorities were welding people inside their homes for purported “public health” reasons and sharing video footage of people allegedly dropping dead in the streets from Covid-19, the critical guidance received from WHO included their Director-General, Tedros Adhanom, stating “in many ways, China is actually setting a new standard for outbreaks“. This was certainly true, but not in any way which deserved to be imitated. Nevertheless, they have been imitated by politicians across the West, intent on proving they “did all that was possible to halt the virus”, at enormous cost across all other public health domains.
Tedros has described Covid-19 as “a new virus”, which is incorrect but widely believed. It is an individuum of existing Betacoronaviruses, against which many of us have immunity providing cross-protection against Covid-19. This is why at least 80% of infections are asymptomatic or only mildly symptomatic. It probably also explains why Covid-19 has very limited impact in large parts of Asia. Cross-immunity between respiratory coronaviruses may limit COVID-19 fatalities.
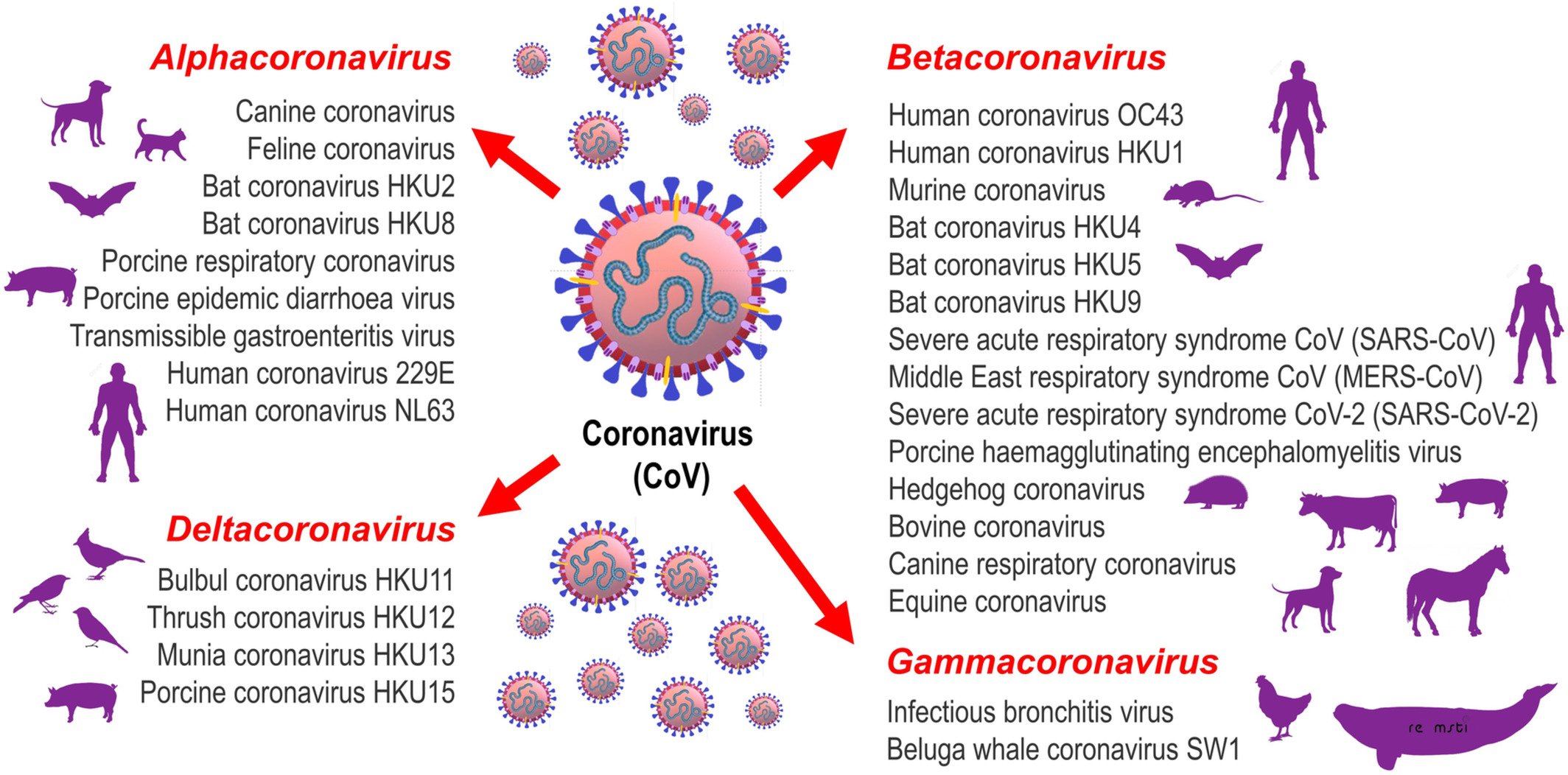
Tedros has also stated that this is the first pandemic caused by a Coronavirus. This is misleading when both SARS and MERS, which caused albeit smaller outbreaks across multiple global locations, are coronaviruses. It is thought that Coronavirus OC43, now an endemic, seasonal common cold virus (as Covid-19 is predicted to become), caused a pandemic in 1889-1890 which was inconclusively labelled as Influenza. Anthony King discusses this in An Uncommon Cold. Nevertheless, it is widely held due to incorrect messaging and consequent hysteria, that there is no immunity to Covid-19 and that it is a unique virus never before seen by the human immune system.
One example of the harms caused by disproportionate pandemic responses is seen in Tuberculosis control, the world’s top infectious killer. Movement restrictions have stopped people requiring treatment for TB from accessing their treatment. This is also the case for many other public health programs such as Malaria, childhood vaccination programs, cancer screening, diagnostic and treatment programs and many others. TB case finding activities have largely ceased. About 75% of the world’s TB control programs are reported to be experiencing significant to moderate disruption. A direct result is that in 2020 we have a 25%-30% reduction in diagnosis of new TB cases. This represents millions of people suffering and dying without access to diagnosis or treatment.
TB program resources have been diverted to Covid-19. People leading TB programs are experts in respiratory infections, so they are often now leading the Covid-19 response in their countries. Instruments used for TB diagnosis have been repurposed and used instead, for diagnosing Covid-19. This has pushed TB diagnosis to a lower priority. The economic impact on countries with limited health resources has also seen TB programs lose funding in favour of Covid-19. People affected by Tuberculosis disease are already often from the poorest and most marginalised communities. Covid-19 pandemic response has made it even more difficult for TB programs to reach these people.
In 2020 both TB and Covid-19 will have killed about the same number of people. However, there are significant differences between the two. Resources and funding towards Covid-19 are many magnitudes more than resources and funding directed towards TB control. There is a handful of vaccines and therapeutics in the pipeline for TB as opposed to the many hundreds being targeted towards Covid-19. TB disease and death impacts people across the lifespan, frequently stealing life from, and causing long term disability in, children and young adults, whilst the average age of impact for Covid-19 is 82yo. The investment in data systems and reporting on Covid-19 is leagues ahead of that for TB. Last month the 2020 Global Tuberculosis Report was published by WHO, reporting on what happened in 2019 for TB. Yet we can follow global data for Covid-19 on a day to day basis from multiple sources. Global Tuberculosis Report 2020: latest status of the tuberculosis epidemic and response.
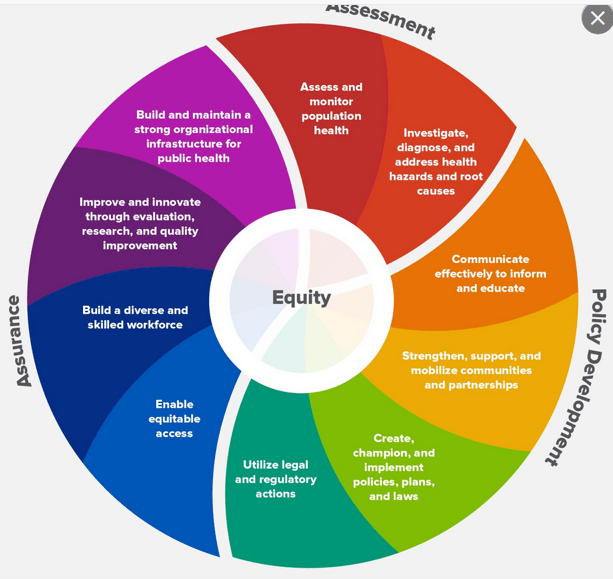
This diagram, taken from Centers for Disease Control : 10 Essential Public Health Services, demonstrates the complexity of public health. There is no single “expertise” in public health, rather it is a multi-dimensional system relying on teams of people from many specialties. The idea that only virologists or epidemiologists can address a pandemic ignores the need for skilled communication, policy expertise, systems expertise, community engagement, sociology and anthropology insights, and many other inputs that virologists and epidemiologists are neither trained in, nor focused on.
It turns out that even cartoonists can be adept at public health artistry. Bob Moran, UK cartoonist, had this to say on Twitter earlier today.
Flu is a serious illness. It kills people. Unlike Covid, it often kills healthy people and even kills children. Flu seasons overwhelm the NHS and can see up to 60,000 excess deaths. Saying Covid is “just flu” makes it sound trivial. No disease is trivial.
But neither is love and neither is freedom. To anyone who disagrees: Think how you are acting right now; unwilling even to shake someone’s hand, see your family or visit your friends, in case you or they are shedding a virus asymptomatically.
And now recall a time when you actually felt ill, had flu symptoms, and still went to work, or to a party, or a wedding. How has your attitude changed so much? Or is it possible that this isn’t you. This isn’t what you think.
This is an illogical groupthink mentality catalysed by a social-media orthodoxy. Viruses are part of our society. It would be nice if they weren’t, but they are. Therefore – just like every other threat we live alongside every day – we ignore them.
We ignore them, not because we want to risk dying, but because we have to risk living. I’m not telling you this because it’s my opinion. I’m telling you this because, until March of this year, it was yours.


Reblogged this on Citizens.
LikeLiked by 1 person