The first identified cases of COVID-19 were detected on December 8, 2019 in Wuhan, China. The first documented case in Europe was reported retrospectively in France, in a patient with pneumonia and positive SARS-CoV-2 PCR result on December 27, 2019.
In January and February 2020 frightening video footage from China flooded social media. People were allegedly dropping dead in the streets from this new, “novel” respiratory virus. At no time in recorded history has falling dead in the street been a phenomenon associated with a virus that takes days to cause symptoms such as breathlessness leaving a patient bedbound.
At no time since this Chinese footage was shared, has any location seen this phenomenon occur again. However, dropping dead in the street as a Covid-19 specific event was etched into human consciousness. A friend in Cambodia retold the story of her neighbour in May last year on a particularly hot day, collapsing in the street near their house. Witnesses became petrified and ran away. Some recorded the event on their phones and posted it to social media. Eventually someone who recognised him went to his aid. He had fainted from dehydration and was soon revived. But the proof was already out, that he had died in the street from Covid-19.
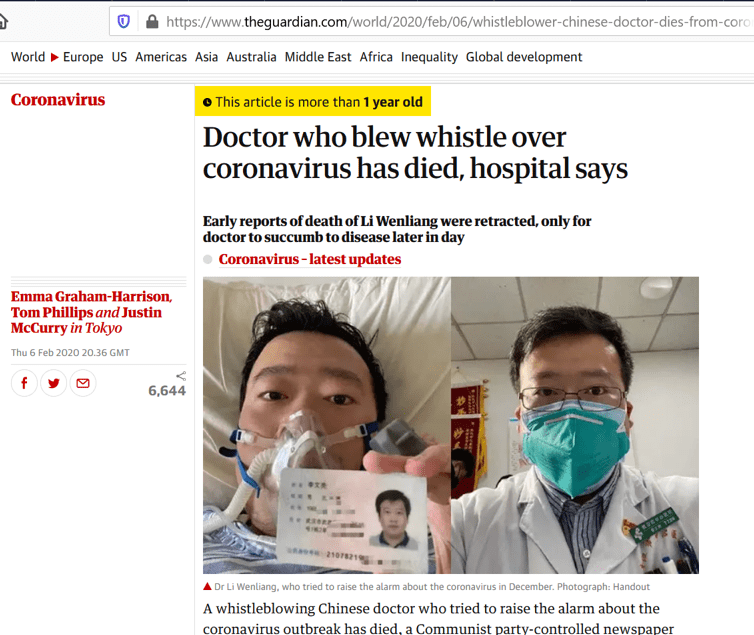
The 33 year old Ophthalmologist who blew the whistle on the new virus circulating in Wuhan reportedly died on 6 February 2020, from Covid-19. Conscious but dying he had time and cause to present his identification for a photograph which made its way to mainstream news sources across western nations; an earlier photograph alongside his deathbed photo shows him double masked more than a year before US CDC (with no supporting evidence) announced double-masking as a new virus control recommendation.
WHO declared a pandemic on 11 March 2020. Director-General Tedros Adhanom Ghebreyesus said “We expect to see the number of cases, the number of deaths, and the number of affected countries climb even higher”. Immediately and synchronously across the globe, a large and sharp peak of deaths occurred. Yet evidence now suggests that SARS-CoV-2 was circulating in Europe as early as September 2019. So why did peak deaths associated with this virus only occur six months later, concurrent to the WHO announcement?
According to physicist and researcher Denis Rancourt, the peak of Covid-19 deaths was unnatural for a number of reasons:
- The peak is too narrow. A viral infection of this type spreading amongst people typically takes 12-14 weeks to peak, not 3-4 weeks;
- Deaths peaked synchronously at the same time across locations which is highly atypical given the multiple variables involved in disease epidemiology across geographical areas;
- Deaths peaked in spring, a time never previously recorded for a death wave of any winter respiratory virus.
In jurisdictions where the Covid-19 peak occurred, there has not been any excess death. Rather, a narrow but high peak of deaths within a tight 4-week timeframe which almost exclusively occurred in people already nearing end of life. Had the sharp peak not occurred, these people would have died within a few months, hence there has been minimal excess death for the year. Evidence is mounting that most excess death is a result of lockdowns rather than Covid-19.
The sharp peak of Covid-19 deaths only occurred in some jurisdictions, who share commonalities which Rancourt has identified as:
- High risk elderly were isolated from families into closed long term care facilities;
- Facilities closed their doors resulting in poor ventilation with consequent increased viral transmission;
- Isolation from family and usual support combined with stress from the fear of a highly publicised pandemic increased the psychological stress of many, which is a well known cause of immune suppression leading to increased rates of disease.
- (Note that he doesn’t touch on the issue of early treatment recommendations for Covid-19 which have since been amended. The death rate for COVID-19 intensive care patients dropped by about one-third by July 2020, due at least in part to better hospital care, a review of published studies found).
These immune suppressed, vulnerable people would have died within months anyway, but human actions made in fear and panic accelerated their deaths. This is especially relevant to the large peak of deaths associated with nursing homes seen in places such as New York, where ill patients were discharged from hospital into care facilities to free up hospital beds for the predicted surge in demand. A similar process occurred in the UK where a significant proportion of Covid-19 deaths have occurred in nursing homes. Other jurisdictions with better procedures more closely aligned to a targeted protection approach (as promoted by the Great Barrington Declaration) did not experience the pandemic in this way.
This demonstrates perfectly, the argument that promoting fear and anxiety in the population as a public health response during a crisis, adds to the damage created rather than providing any kind of solution.
Rancourt goes on to describe further, the response of authorities needing to cover up their erroneous actions by increasing the levels of fear in order to “prove” that the panic was justified. This was achieved by promoting mask mandates, ongoing lockdowns, and all of the associated fear-driven policies which have so confused those of us with experience in infectious disease surveillance and outbreak control who recognised something very wrong transpiring and tried to speak out. The 18 minute interview with Professor Rancourt is available at this link. I also highly recommend the half hour presentation by Nick Hudson summarising the pandemic, which I blogged yesterday.
Voices of reason are slowly starting to win out over voices of panic and fear. Meanwhile however, irrationality continues.




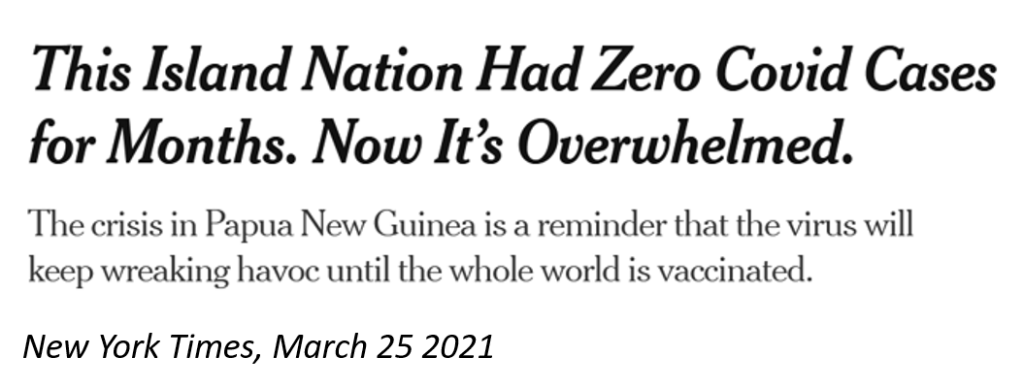
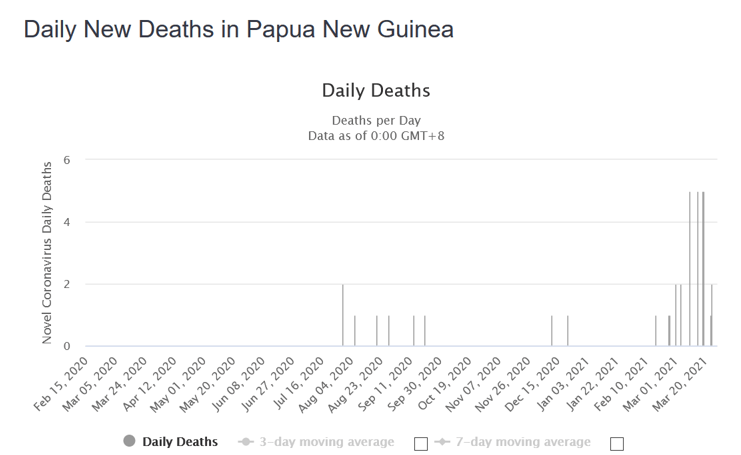
Headlines vs Reality : Papua New Guinea. In an impoverished country with median age of 22yo where the majority of the population die from causes other than old age, it will be difficult to solicit Covid-19 deaths. A similar story is currently underway in Cambodia who have now reached a total of 10 Covid-19 attributed deaths and are instituting punishing measures upon a population with no protections from the ravages of lockdown. Using PCR tests as the benchmark for “disease” and enforcing quarantines and lockdowns, easily overwhelms fragile systems. The perpetual pandemic and associated chaos apparently has no end until the whole world has been vaccinated. This is regardless of risk-benefit analyses which were once a major consideration for all vaccination scheduling.