Professor Sucharit Bhakdi is a retired physician and microbiologist whose career was dedicated to research and teaching. In 2020 he emerged from retirement to express his great concerns about the pandemic response. Since that time he has been “fact checked” alongside so many other eminent scientists, by Bachelor degree graduates employed by the pharma-tech-media industrial complex. The “fact checks” don’t counter Professor Bhakdi’s science, but rather announce various accusations such as “spreading misinformation”.
Bhakdi is a haunted man who has spent nearly three years speaking out against the first-inexplicable, then-sinister actions imposed by those in power, under a guise of “pandemic response measures”. He presents an attempt at lay-friendly science in this half hour presentation, Gene Based Vaccination: Quo Vadis? The Case Against mRNA Vaccines Argued From First Principles of Immunology. “I came back because someone had to say things that are known in the medical text books but have obviously been forgotten“.
WHO recently declared that they intend to introduce mRNA technology for all authorised vaccinations in the world. Doctors 4 Covid Ethics, a global collaboration of doctors and scientists to which Bhakdi belongs, have written a four point memorandum in response, expressing their extreme concerns about this plan. Their four points are summarised as:
- Rationale for development of vaccines:
Benefit must always outweigh risk, which requires that the pathogen is associated with high rates of illness and death; and that the vaccine confers robust immunity against severe disease. - Immunity to respiratory viruses:
Antibodies in the bloodstream do not prevent viruses from entering the cells of the airways. This occurs via a more complicated process, detailed in the memorandum and presentation. - T-cell immunity:
This is required for respiratory infections and is not conferred by mRNA injections. - Gene-based injections are extremely dangerous:
All gene-based injections encoding “non-self” (such as SARS-CoV-II spike protein) have multiple biological dangers to our health, detailed in the memorandum and presentation.
Real life data in populations receiving these injections confirms the concerns which so many doctors and scientists have tried to warn about constantly since the first mention of these substances being used under the name of “vaccines”.
Why are these valid concerns persistently silenced rather than discussed and debated? Another regularly fact-checked eminent scientist is physician and vaccinologist Dr Robert Malone, who summarises here how and why this is happening. The integration of tech, finance, big media and national governments who are now all divisions of one large conglomerate, leads us towards a plan for global Marxist-style control. The philosophy is that resources are finite and are best controlled by a powerful class imposing social credit systems on the majority via digital surveillance. This is being accelerated by the looming financial crisis.
Professor Bhakdi’s excellent lesson in mRNA microbiology, based on the Doctors 4 Covid Ethics memorandum is worthy of half an hour of attention to anyone interested in trying to understand Covid-19 and mRNA microbiology. I’ve added some brief points, which are not representative of the full presentation. The evidence Professor Bhakdi cites is referenced in the memorandum.
- Professor Bhakdi calls on his physician colleagues to understand that most viral pathogens cause self-limiting infections of the respiratory or gastro-intestinal tract, and that severe damage to internal organs caused by bloodstream spread is extremely rare.
- Because airborne viruses are so common, populations across the globe have a high level of background immunity. As such there is no need for vaccine development against most pathogens.
- The surfaces of our mucous membranes (in the airway and gut) are coated with antibodies called secretory IgA (sIgA). Intramuscular injections do not lead to sIgA, which is why the Covid injections were always doomed to fail.
- sIgA are produced by naturally occurring airway infections, which is why the vested agencies (WHO, CDC etc) are now pushing an agenda claiming that we need nasal spray vaccines. But our mucous membranes are already coated with antibodies against common respiratory viruses, which have an “absolutely limited” capacity to prevent infection, which is determined by the quantity we are exposed to (“viral load”). This is why infection with airborne viruses occurs repeatedly throughout our lifespan. Intranasal vaccines will not alter this fact.
- The most common defect in humans is a deficiency of sIgA, and people with this condition do not suffer an excess of respiratory infections. This shows that immunological protection against respiratory viruses does not rest on antibodies, but on T-cells, and also that we have cross-protection at antibody and T-cell levels, against related viruses. [This was shown by the cross protection conferred against Covid from other coronavirus infections such as OC43 and SARS1].
- T-cells are all-important for the initial response to infection. They recognise specific protein fragments which are shared between virus species and other pathogens, and they also recognise proteins which belong to our own cells, which stops them from attacking our own cells (auto-immune disease). T-cells develop in the last month prior to birth, so that babies are born with T-cell immunity and an ability to protect against auto-immune disease.
- We are born with T-cell immunity against coronaviruses, and many other viruses.
- Viral proteins such as the Covid spike protein have multiple fragments, and T-cells are specific to these different fragments. Proteins encoded by virus variants can generate only one to a few different fragments, whilst the other fragments remain the same. As such, cross-protection against a given virus remains robust despite variant evolution.
- Evidence shows that whilst people who have been infected with a previous Covid variant can become re-infected with a new variant, their subsequent infections are never serious.
- Whilst cytotoxic T-lymphocytes (“Killer T-Cells”) bind to specific fragments of a viral protein, antibodies which are generated by T-cell activation, bind to the whole protein. Bound antibodies always trigger activation of the second major arm of the immune system, known as ‘complement’.
- Complement is not well understood, but Professor Bhakdi was involved in the research which discovered how complement kills cells. He describes “killing by killer lymphocytes is silent death; killing by complement is violent death and associated with massive inflammation“.
- Gene-based vaccines do not mimic natural infection. Trained medics should know this because the complement system will attack the individual’s own cells, which are instructed to produce the spike protein. These substances rapidly spread from the site of injection to lymph nodes to the blood, which can transport them throughout the body. [They are known to accumulate in ovaries, testes, heart, liver etc – as described by the Pfizer Trial Data Analysis project]. They can stay in the cells they reach for unknown periods, at least 60 days. This is far more dangerous than natural infection which rarely target lymphocytes or endothelial cells systemically.
- “In stark contrast, each and every gene based vaccine will incite self destructive processes in lymphatic organs and in blood vessels throughout the body. The horrible dangers of self attack events occurring within the immunological network were outlined in [this letter]“. They include reactivation of dormant infections such as shingles, EBV, TB, parasites and many others; the reduced capacity to control new infections which is why people who have been repeatedly inoculated suffer from very serious infections, as their immune system is suppressed; and the activation or reactivation of neoplasms (cancer).
- Concomitantly, concerted immune attack will be mounted against blood vessel walls when the endothelial cells become transfected. This process is illustrated here:
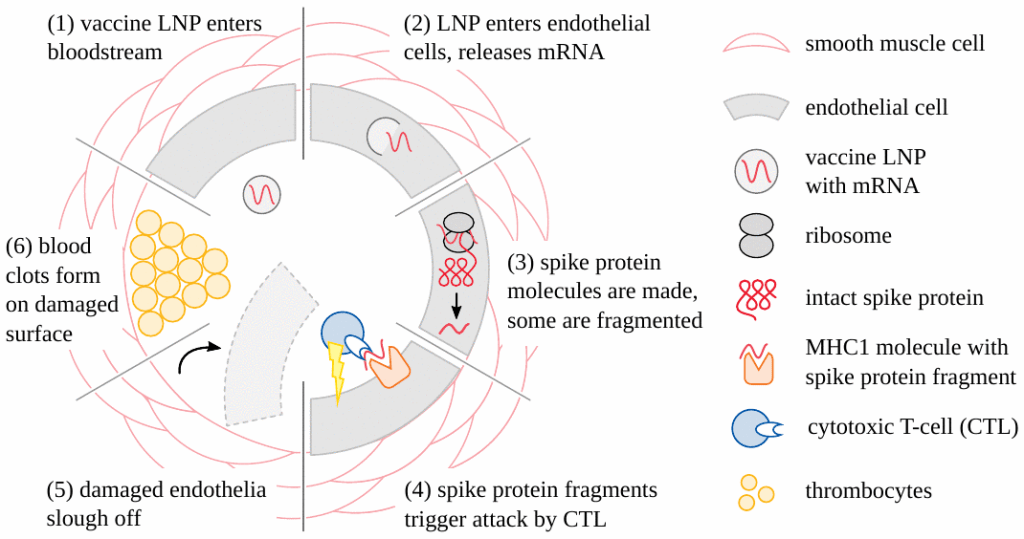
- The alien gene in the endothelial cells leads to an attack by the immune system, allowing the vaccines to leak into tissues: brain, heart, liver; etc etc. Those tissues will then be the seeds of auto-immune destruction: for example hepatitis, thyroiditis, pancreatitis, myocarditis…
- If the liver cells are damaged they can be replaced and repaired, which is true for almost all organs in the body with the exception of the brain and heart, which are permanent damage. First the blood will clot, circulation will stop, second the genes will leak out, leading to cell death which is irreversible in the central nervous system and heart.
- [This information is analagous with what Dr Stephanie Seneff has been warning about with regards to risk for neurodegenerative disease].
- The risk increases with each booster, which increases the violence and efficiency of the auto-immune attack.
- The newest discovery by German pathologists working with Doctors 4 Covid Ethics, published here, shows that vaccine induced spike protein is expressed in the smallest vessels in the brain, leading to necrotising encephalitis.

thank you for summarizing these talks, I am better at understanding if I read than watch. The effects of these gene based, so called therapy, is destroying people’s health, it is frightening, and the governments are still encouraging ‘vaccination’ in Australia.
LikeLike