Seven hours (6 hours 50 minutes) into the one day Lockdown Summit in London yesterday, Dr Peter McCullough dialed in from Texas to present on early treatment for Covid-19. The whole summit was excellent but Dr McCullough, to my mind, stole the show.
McCullough’s CV includes Medical Internist, Cardiologist, Epidemiologist, Professor of Medicine, and internationally recognised authority on the role of chronic kidney disease as a cardiovascular risk state. He has over 1,000 publications and over 500 citations in the National Library of Medicine. Since the pandemic began, he has been a leader in the response to the Covid-19 disaster. He published the first synthesis of multi-drug treatment of patients hospitalised with Covid-19 in the American Journal of Medicine. He has 40 peer-reviewed publications on Covid-19 and comments extensively in the American media on the pandemic response. He has also testified at a number of senate hearings.
Dr McCullough sees patients everyday and has seen or consulted on thousands of Covid-19 patients, and now Covid-19 vaccine injuries. His presentation outlines the approach of outpatient treatment for Covid-19 with the goal of reducing hospitalisations and deaths. He calls this “a giant blunder by public health authorities” globally.
The presentation is largely medical but it’s important information which has been aggressively suppressed throughout the pandemic, at the cost of many thousands of lives, as many doctors have been loudly protesting about – for example, America’s Frontline Doctors and Frontline Covid-19 Critical Care Alliance. Most western countries have alliances like this of medical doctors speaking out in favour of an evidence based and safe response to this virus, against a narrative which has aggressively pushed for vaccination. In Australia Covid Medical Network; in New Zealand Covid Plan B, both of whom are being silenced and accused of “disinformation” in mainstream media, who most people unfortunately continue to assume have no underlying agenda or background influence.

SARS-CoV-2 Infection
There are three major components, being: viral proliferation, cytokine storm and thrombosis.
Dr McCullough outlines each component. Whilst it is a potentially fatal illness, it is long and happens in slow motion. Effective combination treatments are available, but often introduced too late.
Pillars of Pandemic Response
He names four pillars of pandemic response, as:
- Contagion Control (stop the spread)
This is important but the virus is largely unstoppable. - Early home treatment
This presents the only opportunity to reduce spread of the virus, shorten duration and intensity of symptoms, and reduce hospitalisation and death. - Late hospitalisation and treatment
Many times it is too late by this stage, with 38% of patients admitted to ICUs in top US hospitals dying. - Herd immunity and vaccination
He talks about this further on.
Role of Early Ambulatory Treatment
Anti-Spike Protein Antibody Infusions:

These are specific antibodies (the Y shapes) against the spike protein (the spikes sticking out of the virus ball). The antibodies are huge compared to the spike which they are supposed to fit onto, much like a spanner fits onto a nut, and this is an acknowledged limitation of vaccines.
In the USA they have access to an antibody called Regeneron and GlaxoSmithKline monoclonal antibodies, described as a “neutralising antibody cocktail”, which reduce hospitalisations. These were purchased by the US government. Doctors can call to order them, they consist of a one hour infusion in a sterile room, then they go home! This is the treatment President Trump received. Despite a pre-purchase of 500 million doses of this product, they sit on shelves unused as the government provides no information about their availability, instead favouring mass vaccine propaganda.
Hydroxychloroquine:
The most widely used drug for Covid-19 in the world. Why? It reduces viral replication, and this was known from the SARS1 pandemic in 2003. It impairs virus entry into the cell by changing acidity of the endosomes. It works in conjunction with Zinc which inhibits the polymerase that the virus tries to use in the cell entry process. Hydroxychloroquine is also an anti-inflammatory, helping to improve innate immunity.
Because of its effectiveness, Hydroxychloroquine has had the most research undertaken. There have been 259 completed trials, including over 40 randomised controlled trials, with over 4,000 researchers and almost 400,000 patients. All evidence shows that it reduces symptoms, hospitalisations and deaths, when it is started early.
There have been no large randomised controlled trials performed, despite millions of Covid-19 patients providing the ideal setting for large clinical trials in first world countries across the globe, but this has never happened. So we rely on data largely from less developed nations such as Iran.
All of the RCTs which have been undertaken in first world nations have been small and stopped early in “the panic of the pandemic”. Nevertheless, an overall treatment effect is shown.
Ivermectin:
This drug reduces the nuclear entry of the virus once it’s inside the cell, and it also inhibits the dangerous spike protein. “The mechanism of Ivermectin is solid” (which is why anyone following the Covid-19 pandemic story has heard of this drug). There have been 60 completed trials researching Ivermectin, with over 500 scientists and almost 19,000 patients, and the evidence is strong.
One trial, from Dr Pierre Kory, showed that when Ivermectin is used, there is a 71% mortality reduction from Covid-19 disease. It is given as 3 or 5 doses, every other day, with different regimens available. Unlike Hydroxychloroquine, Ivermectin seems more versatile, with effectiveness shown when it is started both early and late in the course of disease.
No single drug completely treats Covid-19 but when drugs are used in combination, as with other fatal infections, treatments are effective. Ivermectin and Hydroxychloroquine are valuable components of combination regimes.
Favipiravir:
Dr McCullough describes this as being “like oral Remdisivir“. It inhibits the polymerase that the virus uses. However, as with Remdisivir, due to the mechanisms involved, it is slow to work. This drug is used in Japan, Russia, Saudi Arabia, Thailand, Kenya and four provinces in India. It has mild effectiveness, and is a distant second to Ivermectin and Hydroxychloroquine. The benefits are that it is an oral drug, with a good safety profile.
Corticosteroids:
Meta-analysis in the use of cortico-steroids, regardless of which (Dexamethasone, Hydrocortisone, Prednisone), suggests a 30% reduction in mortality. Dr McCullough uses Prednisone routinely in his outpatient care of Covid-19 patients.
Inhaled glucocorticoids are also protective and can reduce hospitalisation by up to 87%. This is useful in the early stages of disease, and is effective and safe.
Colchicine:
An anti-inflammatory drug given for 30 days, reduces hospitalisation and death in those who are PCR+.
Anticoagulants:
Drugs such as Aspirin and Heparin show effectiveness against Covid-19 due to the blood clotting that the virus causes.
Putting it all together:
McCullough outlines multi drug treatment regimes which can be used for treating Covid-19, highlighting a study he led with 57 other medical researchers.
He has shared probably over 1,000 studies which support the use of early treatment to reduce hospitalisation and death for Covid-19 disease. He states that vaccination status is not relevant for patients who are at high risk, and that the protocols should be followed for all high risk patients.
_______________
McCullough repeats that no single drug cures Covid-19, but his point is to show the effectiveness and safety profiles of a range of drugs which, used in combination, as for any other infection, reduce hospitalisations and death, which is the ultimate aim.
McCullough recommends the following regime for those with Covid-19 disease. He emphasises that quarantine is only required for those who are sick, and completely unnecessary for those without symptoms. “Doing lockdowns and restrictions on anybody who is not sick is not supported by the data, and in my view fundamentally wrong“. Dependent on symptoms, quarantine can be as short as four days.

He names some of the many medical scientists who deserve credit for this protocol. There are also other protocols, and they tend to be reduced versions of this “full multi-sequenced approach”.
Because it is a long illness, it is a mistake to stop treatments early.
When multi drug treatment is used there is about an 85% reduction in hospitalisation and death from Covid-19. Even in nursing homes, regardless of which protocol is used, when something is done as opposed to nothing, there is about a 60% reduction in mortality.
Presenting this protocol at senate hearings in the USA in January really “crushed our curve” on Covid-19. McCullough presented the protocols at the Texas Senate hearings and it helped them achieve herd immunity.
There are now multiple treatment networks in both the USA and worldwide – this shows a tiny number, including Panda who I volunteer with.

Italy got to zero hospitalisations through their treatment network, Terapia Domiciliare.
Covid-19 Vaccine Safety
There are great concerns over vaccine safety. Many papers have been published on this, demanding review of vaccine safety which has not been done by any government in the world. The multiple clinical concerns include:
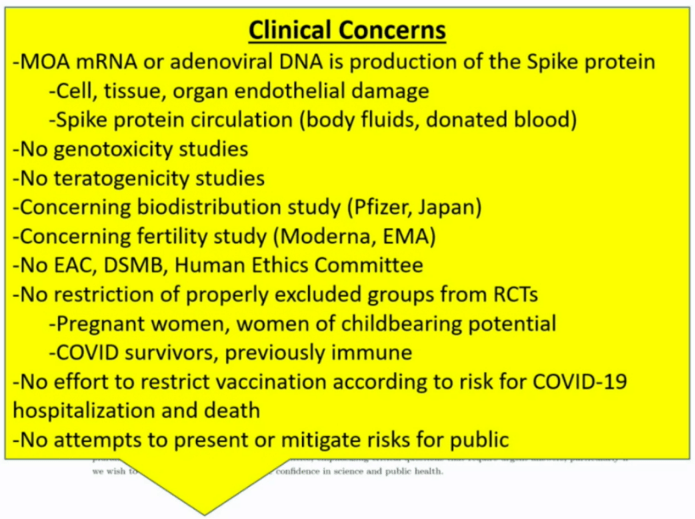
No human ethics committee, no data safety monitoring board, people excluded from the clinical studies are being vaccinated with great harm being done.
This was the USA Vaccine Adverse Events Reporting System data as at 22 January 2021.

And the way this data sky rocketed following Covid-19 vaccine rollout, to 9 July 2021. “There is no doubt about it, the vaccines are showing a very strong signal of mortality“.


“This is a complete and total biological disaster“. Deaths occur almost immediately after vaccination. 86% of deaths in a study by McLachlan et al (Analysis of Covid-19 vaccine death reports from the Vaccine Adverse Events Reporting System VAERS database: Interim Results and Analysis), had no explanation other than the vaccine.
Most deaths occur in the elderly, very quickly post-vaccination. Non fatal and permanent vaccine injuries occur in younger individuals. The vaccines are also failing, with 80% of Covid-19 cases in Israel occuring in the vaccinated.

Dr Tess Lawrie from the Evidence Based Consulting Group in the UK has stated that the vaccines are not fit for human use and should be withdrawn.
An antigen based vaccine called Novavax is coming and may be much safer than the mRNA genetic therapy vaccines being used.
Conclusions

He then fielded some interesting questions from the audience, mainly around vaccine injuries and the issue of treatment and doctors, coordinating vaccine rollouts, not recognising that the vaccines are responsible for serious and probably permanent injury. Some of his replies:
“There is an array of neurological injuries … The non fatal injuries fall under four categories: neurologic, cardiac, immunologic and thrombotic. I have seen them in my practice. We have had 400,000 injuries in the USA and worldwide there are probably millions … I am using low dose Prednisone, and a drug called Fluvoxaimine … Many would also add a course of Ivermectin. It is all completely empiric right now … But we are extremely worried that these neurologic injuries can be permanent …“.
“Patients need to go public in a strong way. Doctors have been completely sold on the vaccine and are refusing to admit that the vaccine is causing injury. Most doctors have taken the vaccine themselves unquestionably and even some doctors now have vaccine injuries … They have to raise public awareness, they have to push very hard to make sure that their points are noted, and their injuries need to be reported to public authorities“.
“Part of this conference is important to spread the word that early treatment works … Ivermectin and Hydroxychloroquine are completely politicised … It can’t be controversial to use a little steroid! … It can’t be controversial to take Aspirin! … I think the suppression of early treatment, which has been uniform, was by design, and I think it was designed to keep people in fear, suffering, and promote hospitalisation and death, in order to get the population to accept mass vaccination. I think the suppression of early treatment and the goal of mass vaccination are closely linked“.
Public Health In Action: when World Health Organisation and other public health agencies don’t do their job, expertise will come from other avenues. Dr McCullough is an exemplary model of genuine public health responding to what seems to be at best, incompetence and at worst, malfeasance.

I have treated over 3,000 COVID patients and Dr. McCullough’s protocol is quite effective although I also used Fenofibrate, cyproheptadine, montelukast, and for older males, Spirinolactone.
LikeLiked by 1 person
Nice website. Thank you for speaking out on this issue. Those of you who are risking your licences are the doctors that the rest of us know we can trust, both clinically and ethically.
LikeLike