As time goes on, the more convinced I become that something seemingly sinister is behind the pandemic response at play through 2020 into 2021, with no apparent end in sight. This is not denial of a virus which has circulated and caused some epidemic level deaths in a number of specific locations. Many locations have not and are not experiencing epidemic levels of anything despite ample opportunity for circulation and detection of the virus. Those locations implementing evidence based public health responses instead of lockdown measures are few and far between, and do so in the face of enormous political pressure to follow the highly bizarre but very popular lockdown narrative.
One example of many possibilities as to why different regions are faring differently, as happens in many diseases, is: In 2010, a virus similar to SARS-CoV-2 was already present in Cambodia. Of course, as with other “successful” lockdown governments, all credit goes to the Cambodian political class and the totalitarian measures they have introduced sweepingly across non-vulnerable settings such as schools, small businesses and young people attempting to feed their families. Cambodia’s population are 85% impoverished. Their city slums are crowded, their rural villages destitute and illiterate, with limited access to even the most basic health care resources. Both the Ministry of Health and NGOs have searched extensively for signs of Covid-19 disease across the nation, but there is no increase in respiratory disease or excess mortality. They continue to experience small clusters of PCR positive test results with almost no associated disease and zero deaths. The chances that the political class from their city mansions, luxury cars and second homes in western nations has suddenly contributed effectively to reduce a single disease whilst all other infectious diseases of poverty continue to circulate without adequate services to meet need, are zero. Yet for some highly bizarre reason it is widely believed that there could be no other epidemiological explanation than “successful lockdown measures”. The standard global narrative is that an intervention with no evidence supporting it as a public health measure is why countries are not experiencing epidemic levels of virus. Not virus characteristics. Not population characteristics. Not environmental characteristics. This is not public health. The aggressive silencing of genuine public health is politics and power driven by lockdown beneficiaries promoting fear and feeding on the naiivety of many.
HART (Health Advisory Recovery Team) in the UK have started a weekly bulletin to combat the myriad news reports of terror upon terror keeping people locked up in their homes and living in constant fear. The second edition published on 19 February begins:
COVID-19 in context
With every death comes personal tragedy, nevertheless it is important to remember:
– The median age of at death with COVID-19 (around 82 years) exceeds normal life expectancy.
– The majority of those who died with the virus also had two or more serious, chronic illnesses.
– In 2020, there were 388 COVID-19 deaths in those aged 60 and under with no prior illnesses.
– 99.9% of people under 70 years and with no underlying conditions survive the virus.
Usually such information would be made widely available by functioning public health units offering sensible, contextualised information for the general public in order that people could make appropriate decisions about their own level of risk and circumstance; with sensible infection control policies for high risk settings such as hospitals and long term care facilities. Instead, people of all ages and circumstances are being forced to remain in their homes, facing unemployment, small business closure, bankruptcy, mental health crises and their children losing precious socialisation and education opportunities. There are toddlers today who have no experience of meeting or playing with other children. This has a significant impact on long term childhood development outcomes. In poor countries the sacrifice includes starvation. In many countries the sacrifice includes reduced access to health care for other life threatening conditions. In the UK and probably elsewhere, it includes the elderly and infirm in long term care facilities, reliant on social contact as a health protection measure, left in strict isolation for many months leading to exacerbation of conditions such as dementia. Excess death from non-Covid causes is rising steadily in many places. Yet, research shows “no clear, significant beneficial effect of (more restrictive) non-pharmaceutical interventions on (Covid-19) case growth in any country“. This is not public health.

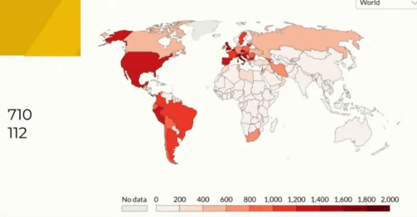
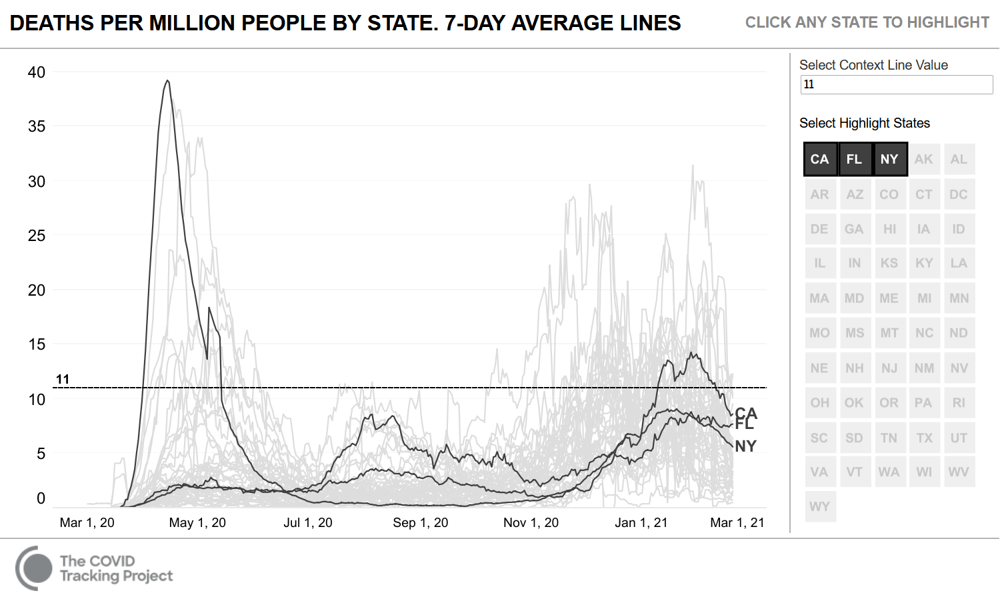
Sweeping lockdowns have been implemented in California and New York for almost a year, compared to Florida who ceased lockdowns after Governor Ron DeSantis consulted with Great Barrington Declaration advisors in September 2020. Covid-19 associated data for these three states is shown below. Florida has the second eldest population in the nation (after Maine); California has the 45th eldest population and New York has the 26th eldest population. California and New York remain in varying levels of lockdown, with playgrounds cordoned off, homelessness rising exponentially, high streets empty, children locked down at home and a severe mental health crisis playing out in the form of increased overdose deaths and suicides. This is not public health. By comparison Florida are open and functioning, their children are in school and their small businesses are trading whilst their public health policies focus on evidence based recommendations such as targeted protection of the vulnerable.
I find myself agreeing with Australia’s previous Liberal Party MP Alexander Downer on the fate that awaits Australia if they continue to pursue a ZeroCovid policy via ongoing, unpredictable, sweeping lockdowns. Why are the government pursuing this approach instead of seeking evidence based public health solutions? What of the possibility of prior immunity, environmental influences or prior circulation of similar Coronaviruses influencing the very different epidemiology seen in Australia compared with Europe and America? What of protecting the vulnerable whilst allowing society to continue to function, as World Health Organisation’s systematic review of evidence for appropriate pandemic response recommended?

Xi’s Infectious Model is the third instalment of a short film series by Kate Wand, based on a letter by an international team of professionals, researchers and activists, calling for an expedited investigation into scientific fraud in public health policies.
A brief but impassioned reminder here from Dr Roger Hodkinson in Canada, that this is politics playing public health. What could possibly be driving such a nonsensical, single-narrative, closed-discourse, oppressive and non-evidenced pandemic response right across the globe? Why have so many of us, with numbers increasing daily, felt gaslighted by some of the biggest public health agencies in the world? What is the link between Covid-19 and Swine Flu in 2009? The answers are convoluted but all roads seem to lead to power, profits and politics. Not public health.

Reblogged this on Citizens.
LikeLiked by 1 person