This week’s media misrepresentation includes “Fears of catastrophe as rising Covid-19 cases hit Papua New Guinea’s stretched health system“. “Plunged into a Covid-19 crisis“, “temporary beds are filling up fast with seriously ill patients“, “health workers are being particularly affected, prompting fears that services may be crippled“, “a new coronavirus tragedy is just starting to unfold on Australia’s doorstep“. These photographs showing three young looking, masked patients all in varying relaxed poses apparently support the alarm.


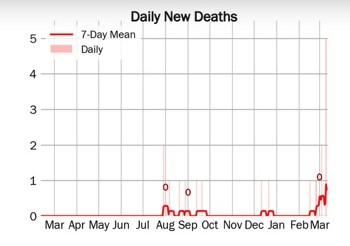
Papua New Guinea have had twenty one deaths in people who tested PCR positive to Covid since the beginning of the pandemic. Five of them occurred in a single day this week, hence the media alarm. The median age of Papua New Guinea’s population is 22 years old. Each year the nation reports around 30,000 Tuberculosis diagnoses, about 4,000 of whom are estimated to die from TB disease, or about 330 TB deaths per month.
People in impoverished countries like Papua New Guinea and Cambodia are living in fear and being forced to stay off the streets. As well as not being a public health intervention supported by any evidence, this is not a realistic thing to require of millions of people whose day to day lives play out in the streets selling, trading, or offering services for a tiny daily fee which they require for survival. With limited health literacy and no access to alternative information people are afraid. The public health implications of this type of response are cataclysmic. This is the famine of biblical proportion predicted by the United Nations a year ago, accelerating.
Cambodia reported their first death this week from Covid-19 almost 14 months after the first case was diagnosed in a man from Wuhan in January 2020. They are locked down today, with reports of usually bustling streets completely empty. Government have widely broadcast preparations of a Covid-19-dedicated crematorium and the new laws associated with their predictions of pandemic level deaths in a population with a median age of 25 years old. Anyone who dies with Covid-19 will be required to be cremated, unless for religious reasons they prefer burial. This seems a strange thing to have to announce given that it basically describes current funeral practices. Anyone who “willingly” transmits Covid by breaking lockdown laws will face between five to twenty years in prison; fines for not wearing face masks are US$50 to US$250 (unaffordable for most, with fines for various infringements already a feature of everyday life which visibly enriches law enforcement workers whilst simultaneously maintaining poverty of the masses); and anyone heard speaking against government pandemic narrative will face a lifetime of debt in the form of fines, or a severe jail sentence.
Most impoverished nations are led by totalitarian rule. Pandemic lockdown is a compatibly oppressive accessory, especially as it confers further transfer of wealth to the ruling classes. Promoting global fear of an infectious disease and “lockdown” as a public health intervention was always going to result in cataclysm for the world’s poorest. This is not public health yet it came directly from World Health Organisation, advising against their own evidence based guidelines.

Canadian Epidemiologist Bruce Aylward speaking in Beijing on 24 February 2020. The briefing transcript is available at this World Health Organisation document. Thirteen days later lockdown was imposed in Italy on March 9, the first western domino to fall, with many falling soon after. A few weeks later Aylward was questioned about Taiwan by a Hong Kong news agency. Taiwan are currently excluded from WHO membership under the “One China” policy, indicating Beijing’s authority within the agency. The interview did not go well, as this two minute video shows.
Another example of the strategy of fear being used has been reporting of disease fatality rates. These can be reported in different ways, depicted by this diagram. Deaths divided by diagnosed (cases) provides a case fatality rate (CFR) whilst deaths divided by infections provides an infection fatality rate (IFR). Deaths divided by population provides the population fatality rate (PFR), which is often presented as “per 100,000” people.
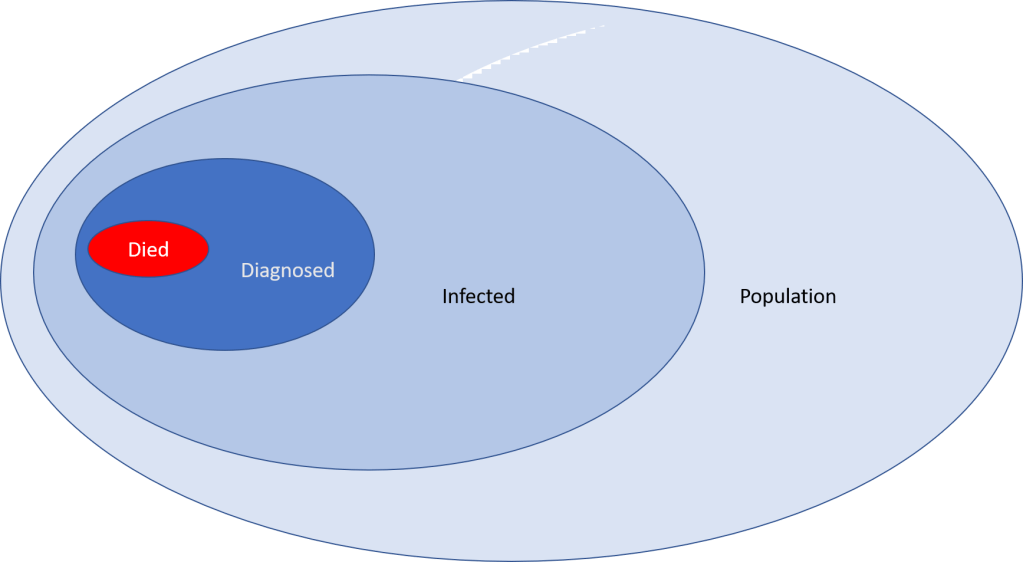
The number of people diagnosed with an infectious disease, particularly a highly transmissible respiratory virus which often presents as mild symptoms meaning people don’t seek diagnosis, is always significantly less than those who are actually infected. As such the case fatality rate is always much higher than the infection fatality rate, where the number who died is a much smaller fraction of the denominator.
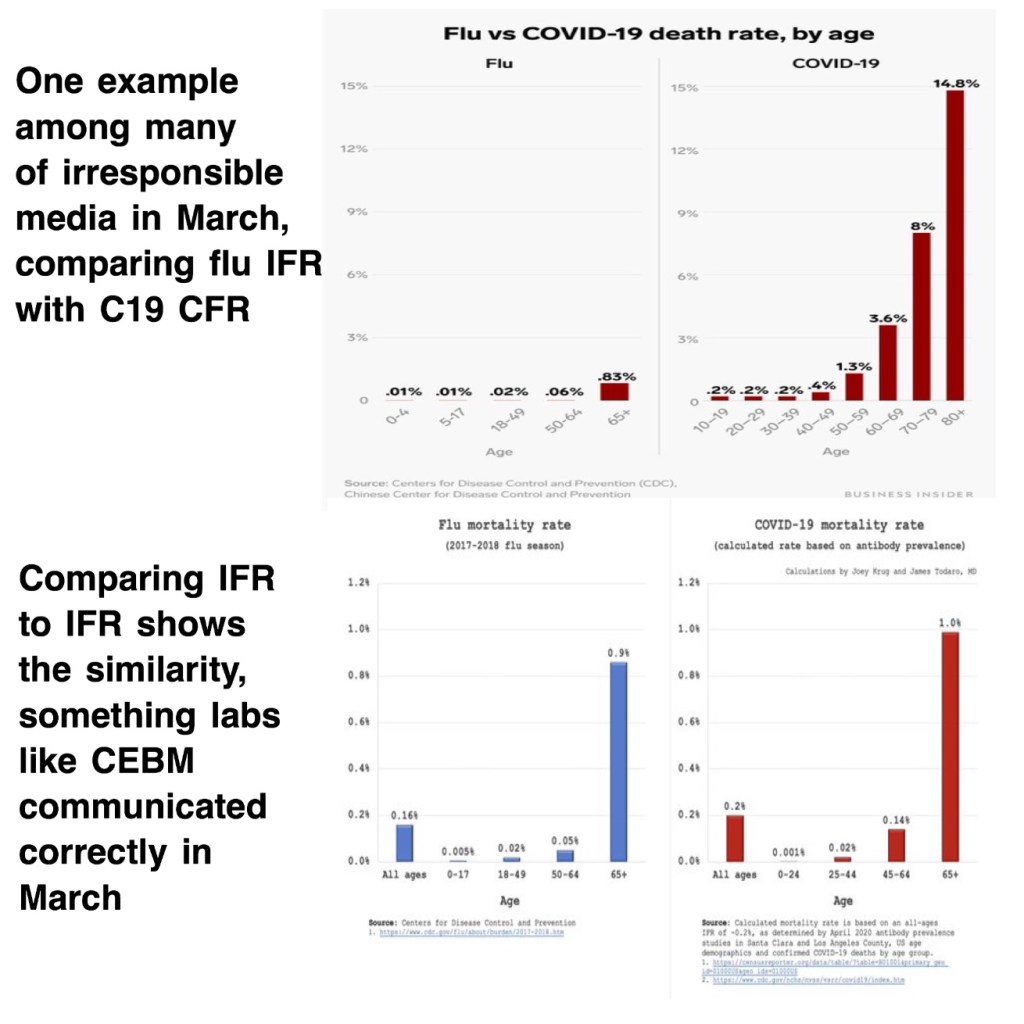
In the past year a common reporting error, perhaps unintentional although agencies such as CDC and WHO have skilled public health staff who must surely know the difference, has been to compare Influenza infection fatality rates with Covid-19 case fatality rates. Dr Mark Changizi, a scientist speaking out vociferously against the dishonesty and mass hysteria characterising this pandemic, highlighted a report in Business Insider in March 2020 which compared Influenza IFR (a lower rate) with Covid-19 CFR (a much higher rate). His reference to CEBM is Oxford University’s Centre for Evidence Based Medicine, one of the most reliable, evidence based public health resources available. He corrected Business Insider’s information as below, stating that the fatality rates are “about the same. Safer than flu for young, a nasty flu for old“.
Every single fearful media report deserves to be questioned, examined and interrogated before being blindly believed. Every single expert too. Becoming a sceptic might protect not only ourselves, but the world’s most vulnerable.

